

Patient presentation
a 24-year-old healthy female with no medical history presented to our emergency department (ED) with complaints of trouble swallowing for the past 2 months and mild anterior neck discomfort. She described an occasional feeling of food getting stuck in her esophagus causing her to force vomiting to feel better. She denied sore throat, fever or chills, cough, recent illness, sick contacts, chest pain, shortness of breath, recent weight loss, or other complaints.
Vital Signs in the ED were: BP 108/74 mmHg, temperature 36.70C, pulse 88 beats/min, respirations 16 breaths/min, and pulse oximetry 99% on room air. Her physical exam was unremarkable.
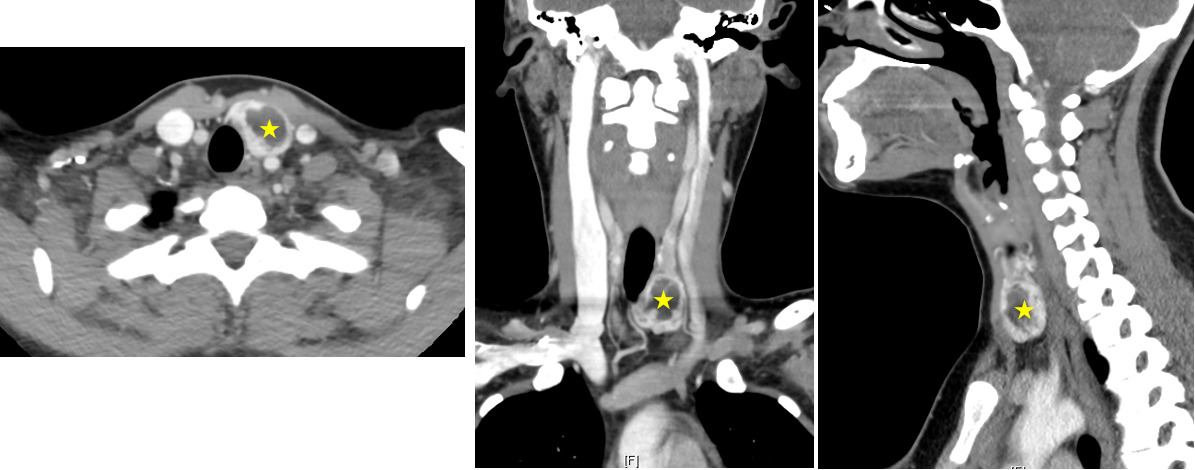
A neck computed tomography (CT) scan with contrast showed an enlarged left thyroid gland with a heterogeneous hypodense nodule measuring 1.9 x 1.1 x 2.3 cm. The left thyroid lobe was seen to be abutting the anterior upper esophageal wall without significant mass effect on the trachea, esophagus or vascular structures of the neck (Figure 1). The patient also had a smaller, sub-centimeter hypodense nodule in the right thyroid lobe.
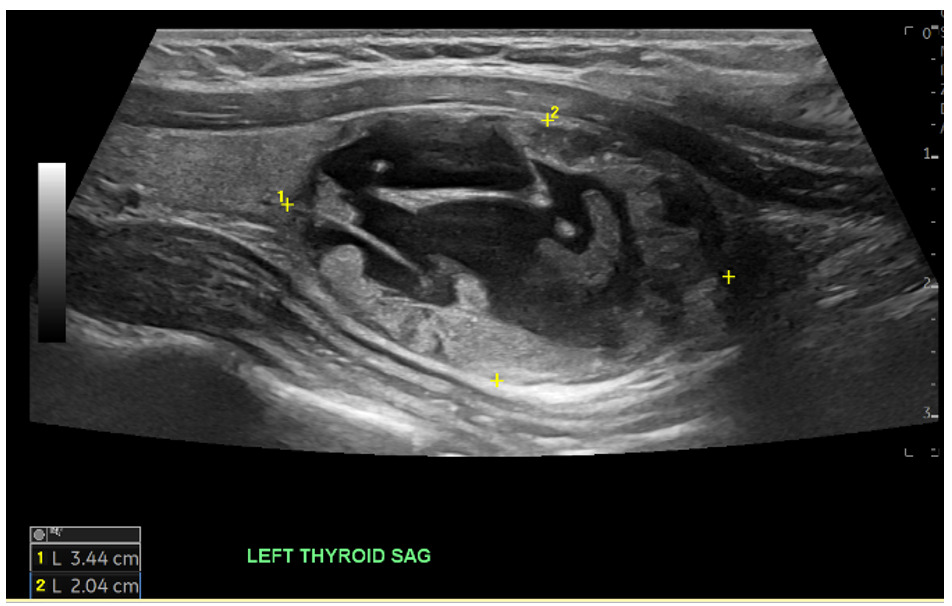
A thyroid ultrasound demonstrated a large cystic and solid nodule in the left thyroid measuring 3.4 cm in largest dimension categorized as TR 3 as well as a right thyroid nodule categorized as TR 4 per Thyroid Imaging Reporting & Data System (TI-RADS) criteria (Figure 2). Labs showed no significant abnormalities.
The patient was discharged home after a discussion of the results and referral for a non-emergent outpatient follow-up with otorhinolaryngology for an outpatient fine needle biopsy (FNA). At 6-week phone follow-up, the patient reported that FNA revealed a benign thyroid nodule.
Diagnosis
Thyroid nodule
Discussion
According to the American Thyroid Association, a thyroid nodule is defined as a discrete lesion that is distinct from the surrounding parenchyma within the thyroid gland.1 The American College of Radiology TI-RADS classification is based on five criteria: composition, echogenicity, shape, margin, and echogenic focus. A TR3 is considered mildly suspicious and an FNA is recommended if the diameter is >2.5cm. A TR4 is considered moderately suspicious, and an FNA is recommended if diameter is >1.5 cm.2 Fortunately, the thyroid in our patient was of benign etiology.
Ethical considerations
Written informed consent was obtained for the publication of these clinical images and accompanying case details.