
Patient presentation
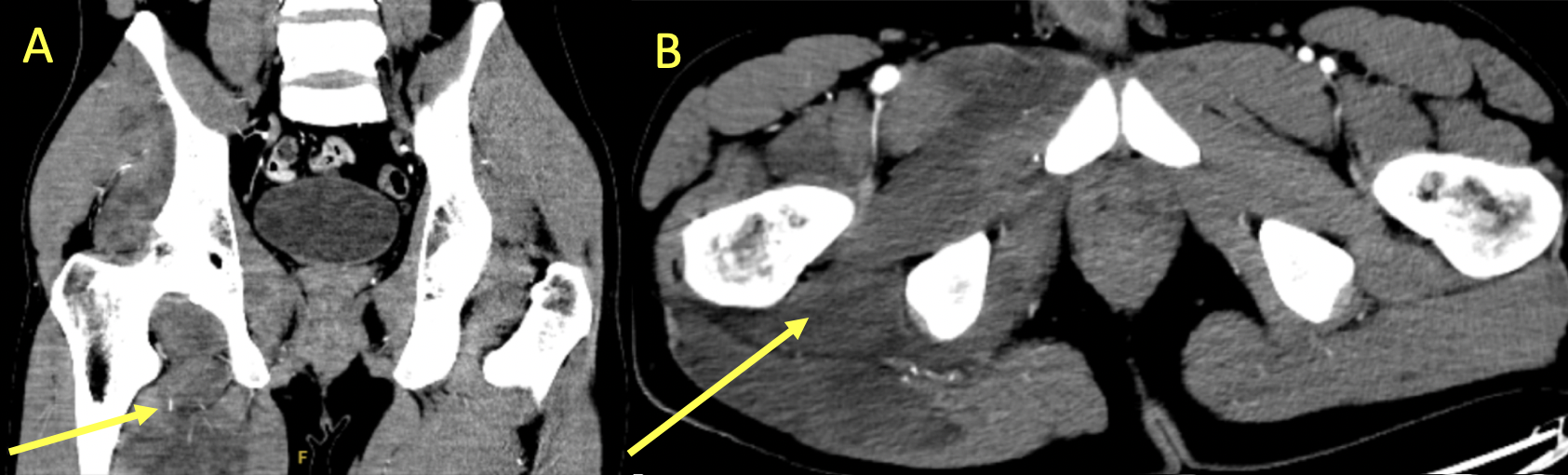
A 25-year-old male presented with atraumatic right-sided flank and thigh pain with an onset of 3 hours ago. He had limited right hip mobility and strength. Studies showed creatinine kinase (CK) 73,218 U/L, potassium 5.7 mEq/L, and BUN/Creatinine 34/1.6 mg/dL. CT imaging revealed edema in multiple muscle groups [Figure 1]. MRI confirmed extensive myositis [Figure 2]. The patient was aggressively hydrated and started on intravenous methylprednisolone to reduce inflammation. He ultimately recovered to baseline and was discharged.
_and.png)
_and_stir_(short_tau.png)
Diagnosis
Atraumatic unilateral myositis with rhabdomyolysis of the right lower extremity
Discussion
Rhabdomyolysis describes the breakdown of muscle, causing a release of muscle cell contents into the bloodstream, leading to electrolyte disturbances and acute renal failure from myoglobinuric intratubular cast formation.1,2 Whereas myositis involves muscular symptoms with elevated CK, diagnosis of rhabdomyolysis requires a CK elevation greater than five times the upper limit of normal.1,2
Atraumatic flank and extremity pain are often attributed to urolithiasis and sciatica. A high index of suspicion can facilitate assessment for rarer etiologies such as rhabdomyolysis.2 In our case, the patient admitted to recent use of cocaine and amphetamine, which can increase muscle activity and lead to excessive energy demands.2,3 Although this points towards rare drug-induced myositis, the patient was responsive to steroids given for refractory pain, suggesting a possible autoimmune etiology.4 CT and ultrasound can visualize rhabdomyolysis as focal hypodensities and muscle with both decreased and increased echogenic areas, respectively.5 Although nonspecific, MRI visualizes increased signal intensity with a sensitivity as high as 100% compared to 62% and 42% in CT and ultrasound, respectively.5 Treatment of rhabdomyolysis involves IV hydration to prevent and treat acute kidney injury.1
Ethical considerations
Written informed consent was obtained for the publication of these clinical images and accompanying case details.