Introduction
Epidemiology and Clinical Burden
The prevalence of IPF varies based on geographic region. In Europe, prevalence is estimated at 10-40 per 100,000 patient years [1]. North America, Asia and Australia have a prevalence of 14-59, 5-40 and 32-35 per 100,000 patient years respectively.1 In addition, IPF has a high clinical burden in affected patients. Median survival is only estimated to be 3-5 years even when using antifibrotic therapy.2
Diagnostic Criteria and Features
IPF is a progressive interstitial lung disease (ILD). Diagnosis requires exclusion of other ILDs and a usual interstitial pneumonia (UIP) pattern on high-resolution chest CT (HRCT) or specific patterns and histopathology in biopsied patients.3 HRCT features of UIP include subpleural and basal predominant distribution and honeycombing with or without bronchiectasis.4 IPF should be suspected in adults with exertional dyspnea, cough, crackles, and finger clubbing.4 IPF is rare in adults under 50 and commonly presents in the 6th or 7th decade and is more common in men and smokers.4
Pathophysiology
IPF is driven by abnormal wound repair due to recurrent alveolar epithelium injury from various factors (genetic, environmental, immunologic, etc.) [5]. This leads to metabolic dysfunction and cellular senescence. Injured cells activate profibrotic signaling, recruiting fibroblasts and myofibroblasts, resulting in excessive extracellular matrix deposition.5 Furthermore, single-cell RNA-sequencing has identified epithelial cell populations promoting a profibrotic state.5 Antifibrotic therapies like nintedanib and pirfenidone are based on these insights, targeting fibroblast proliferation and collagen synthesis, respectively, to manage IPF progression.5
Mechanisms of Antifibrotic Drugs
Nintedanib inhibits tyrosine kinases (PDGF, FGF, VEGF receptors), decreases ECM proteins (fibronectin, collagen 1a1), induces fibroblast autophagy, and interferes with fibrosis processes (proliferation, migration, differentiation, protein deposition). Animal studies show its anti-inflammatory and anti-fibrotic activity in lung fibrosis models.4,6,7
Pirfenidone disrupts IPF mechanisms by interfering with TGF-β signaling, impairing SMAD3 and phospho-p38 phosphorylation. It inhibits PDGF and FGF, preventing fibroblast to myofibroblast transformation, and exhibits anti-inflammatory effects by suppressing dendritic cell activation and reducing chemokine and cytokine production. This has raised interest in its potential for treating non-pulmonary diseases like HFpEF.8
Research Gap
Current guidelines do not preferentially recommend one agent over the other due to limited comparative evidence. Previous reviews included Phase II trials or observational data, which may confound outcomes due to differences in dosing, follow-up, or patient selection. This study aims to provide the first network meta-analysis (NMA) restricted to Phase III trials to compare pirfenidone and nintedanib on clinically relevant endpoints (FVC decline, mortality, exacerbations, and tolerability).
Rationale for Phase III Focus
Phase III trials were selected to ensure standardized dosing, rigorous endpoints, and adequate power, whereas Phase II trials (e.g., TOMORROW for nintedanib) often use exploratory outcomes or smaller cohorts, introducing heterogeneity.
Methods
Inclusion Criteria
Phase 3 randomized controlled trials enrolling adults aged 18 years or older with a confirmed diagnosis of idiopathic pulmonary fibrosis (IPF) were included in this study. Eligible studies compared treatment with either pirfenidone or nintedanib against placebo. Trials were required to report at least two of the three clinically relevant outcomes, including a ≥10% decline in forced vital capacity (FVC), one-year all-cause mortality, acute exacerbations or hospitalizations, or treatment discontinuation due to adverse effects. Only studies with completed follow-up and publicly available data by July 2025 were considered. Publications were restricted to those available in English.
Information Sources
We systematically searched major bibliographic databases (e.g., MEDLINE, Embase, and Cochrane Central Register of Controlled Trials) and clinical trial registries for randomized controlled trials (RCTs) evaluating nintedanib or pirfenidone versus placebo in patients with IPF. The search included studies from database inception through the latest available date and used combinations of keywords and controlled vocabulary terms related to “idiopathic pulmonary fibrosis,” “nintedanib,” “pirfenidone,” and “randomized controlled trial.” The full search strings are provided in supplementary appendix A.
Study Selection
We included parallel-group, randomized, double-blind, placebo-controlled trials that enrolled adults with a diagnosis of IPF according to contemporaneous guideline criteria, and that evaluated either: Nintedanib versus placebo, or Pirfenidone versus placebo.
To ensure comparability across trials, key inclusion criteria required: IPF confirmed by multidisciplinary discussion and/or high-resolution computed tomography consistent with a usual interstitial pneumonia pattern, with or without histopathologic confirmation. Baseline lung function parameters within typical trial ranges (e.g., forced vital capacity [FVC] and diffusing capacity of the lung for carbon monoxide [DLCO] thresholds as defined in each protocol). Minimum follow-up of approximately 52 weeks or closest available to 1 year.
We excluded non-randomized studies, open-label extensions, and single-arm trials. Trials of other investigational antifibrotic or immunomodulatory therapies without a nintedanib or pirfenidone arm were also excluded. Finally, studies that did not report at least one of the prespecified primary or secondary outcomes were similarly excluded.
Based on these criteria, four pivotal trials formed the evidence base for the network: INPULSIS-1 and INPULSIS-2 (nintedanib vs placebo) and ASCEND and CAPACITY-004 (pirfenidone vs placebo).
Data Collection Process
The data for each of the included studies was extracted using the Cochrane Data Extraction and Assessment Form. The extracted variables included trial name, publication year, intervention and comparator, sample size, patient characteristics, follow-up duration, definitions of study outcomes and event counts or summary effect data for each outcome. For multiarm or companion trial programs, data were extracted in a way that preserved the randomized comparison structure while avoiding double counting.
Assumptions Made
For trials that reported outcome data only as percentages, corresponding integer event counts were derived by multiplying the reported percentage by the total sample size for each treatment arm and rounding to the nearest whole number. In the ASCEND trial, acute exacerbations were not explicitly reported; instead, respiratory hospitalizations were provided and were therefore used as a proxy measure for acute exacerbations. Finally, we assumed that key potential effect modifiers—including baseline forced vital capacity (FVC), age, and underlying comorbidities—were similarly distributed across treatment groups, thereby minimizing confounding across comparisons.
Risk of Bias Assessment
The Cochrane Risk of Bias 2.0 tool was used. 5 domains were assessed in this tool: randomization, deviations, missing data, measurement and reporting bias. Each study had its domains scored individually and received an overall score of low concerns for bias, some concerns for bias, or high concerns for bias. Finally, the entire body of evidence received a general score. Because all included studies were phase III randomized placebo-controlled trials, overall risk of bias was expected to be low to moderate, although outcome-specific differences in reporting and event ascertainment were considered in interpretation.
Outcomes
The primary outcome was clinically meaningful decline in lung function, defined as a relative decline in FVC of at least 10% from baseline at 1 year (or nearest reported time point). This threshold is widely used as a surrogate marker for disease progression and has prognostic significance in IPF.
Secondary outcomes included all-cause mortality at 1 year, acute exacerbations of IPF as defined in the individual trial protocols and treatment discontinuation for any cause, as a pragmatic measure of overall tolerability and adherence.
Effect Measures
All outcomes of interest were treated as dichotomous outcomes. All dichotomous outcomes were summarized using risk-ratios (RR) with corresponding 95% confidence intervals (CIs).
Synthesis Methods
We calculated risk ratios (RRs) and corresponding 95% confidence intervals (CIs) for each outcome within each trial, comparing active treatment (nintedanib or pirfenidone) with placebo. These trial-level RRs formed the input for the network meta-analysis.
A Bayesian network meta-analysis was conducted to estimate both treatment effects versus placebo for each agent, an indirect treatment effects for pirfenidone versus nintedanib.
The network was structured with placebo as the common comparator, creating a simple three-node network (nintedanib–placebo–pirfenidone). We used a random-effects model to account for between-study heterogeneity in treatment effects, recognizing that trial populations and designs, while similar, are not identical.
For descriptive assessment of heterogeneity within treatment comparisons, we examined between-study variance (τ², tau-squared), the I² statistic to quantify the proportion of total variability due to heterogeneity and the Cochrane’s Q test to assess statistical evidence of heterogeneity.
A DerSimonian–Laird random-effects model, implemented using the netmeta package, was used to generate frequentist estimates of heterogeneity and to facilitate interpretability for clinicians familiar with traditional meta-analytic measures. These heterogeneity estimates were considered alongside the Bayesian network meta-analytic results to provide a comprehensive assessment of consistency and uncertainty.
All analyses were performed using RStudio (R Foundation for Statistical Computing), employing established packages for pairwise and network meta-analysis. Statistical significance was defined as a two-sided p-value < 0.05 for frequentist tests, and Bayesian credible intervals not crossing unity for RRs were interpreted as evidence of a treatment effect.
Reporting Bias Assessment
Comparison adjusted funnel plots could not be used in this network meta-analysis due to the number of studies being less than 10. Therefore, our ability to assess for reporting bias is limited to the certainty of evidence assessment.
Certainty of Evidence Assessment
Evidence certainty was assessed for each outcome of interest and the entire body of evidence using the GRADE criteria. 4 domains were assessed: inconsistency, indirectness, imprecision and publication bias. Each study was evaluated and graded on each domain and was assigned a low, moderate or high certainty of evidence. The entire body of evidence was subsequently assigned a similar score as well.
Results
Study Selection
PRISMA flow diagram is included in the supplementary appendix B.
Study Characteristics
A total of 4 phase III randomized controlled trials were included in this study. In trials INPULSIS-1 and 2 treatment arms were randomized 1:1 to either treatment N=309 and N=329, respectively) or placebo groups (N=204 and N=219) for 52 weeks [9,10]. Nintedanib 150mg was administered to the treatment group [9,10]. Across both trials, mean age was 66-67 years and 75% of patients were male [9,10]. Mean baseline FVC was 79% of the predicted value.9,10 In the ASCEND trial, a total of 555 patients were randomized to either Pirfenidone 2403 mg/day (N = 278) or placebo (N = 277) for 52 weeks [11]. The mean age was 67 years and 74% were male. Mean baseline FVC was 67.8±11.2% of the predicted value in the pirfenidone group and 68.6±10.9% of the predicted value in the placebo group.11 In the CAPACITY-004 trial, a total of 435 patients were assigned to Pirfenidone 2403 mg/day (N = 174), Pirfenidone 1197 mg/day (N = 87) or placebo (N = 174).12
A summary of the trials, their characteristics and their respective results can be seen in supplementary appendix C.
Risk of Bias
Risk of bias was assessed across all included studies using standard domains. All trials employed appropriate random sequence generation and allocation concealment procedures to assign participants to treatment or placebo groups, resulting in a low risk of bias related to randomization. Deviations from intended interventions were minimized through the use of double-blind designs across all studies, thereby reducing the likelihood of performance bias. Missing outcome data were minimal, with less than 15% attrition in both treatment and control arms in every trial, suggesting a low risk of bias from incomplete outcome data. Outcomes were measured by blinded investigators using standardized assessment protocols, supporting a low risk of detection bias. Finally, all studies were prospectively registered and reported prespecified endpoints consistently, indicating a low risk of selective reporting. Overall, the total body of evidence was judged to have a low risk of bias.
Synthesis Results
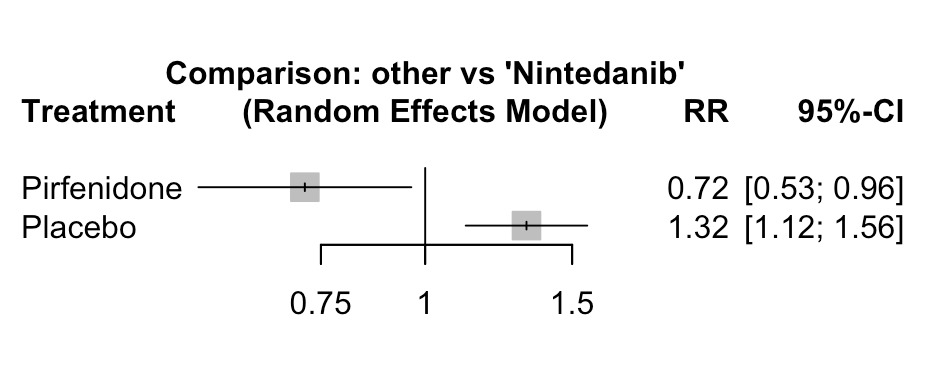
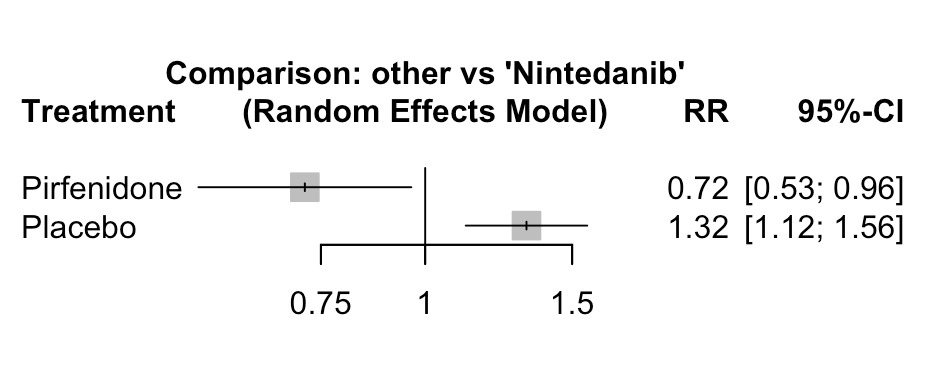
≥10% FVC Decline: All four trials reported data on ≥10% FVC decline from 52-72 weeks. In the random-effects network meta-analysis, both pirfenidone and nintedanib significantly reduced the risk of FVC decline when compared to placebo: nintedanib had an RR of 0.76 (95% CI 0.64–0.89; p < 0.001), and pirfenidone had an RR of 0.54 (95% CI 0.43–0.69; p < 0.001). Indirect comparison showed pirfenidone to be superior to nintedanib (RR 0.72; 95% CI 0.53–0.96; p = 0.027). Heterogeneity was negligible (I² = 0%, τ² = 0; Cochran’s Q p = 0.43), indicating consistent effects across studies.
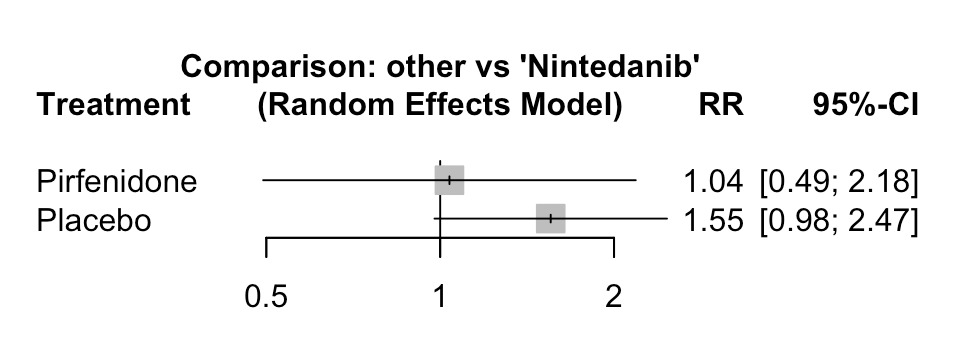
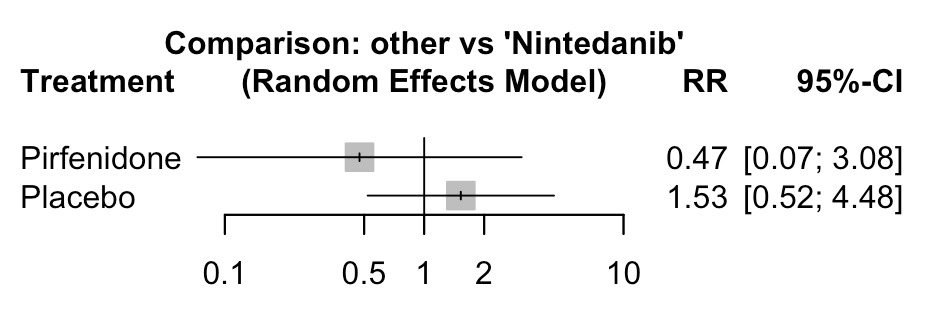
All-cause mortality: All 4 trials reported data contributing to all-cause mortality at one year. Neither pirfenidone or nintedanib significantly impacted mortality when compared to placebo. nintedanib’s RR was 0.64 (95% CI 0.40–1.02; p = 0.06), and pirfenidone’s RR was 0.67 (95% CI 0.37–1.19; p = 0.17). Indirect comparisons between these two agents yielded an RR of 1.04 (95% CI 0.49–2.18; p = 0.92). Between-study variability was low (I² = 0%, τ² = 0; Q p = 0.91).

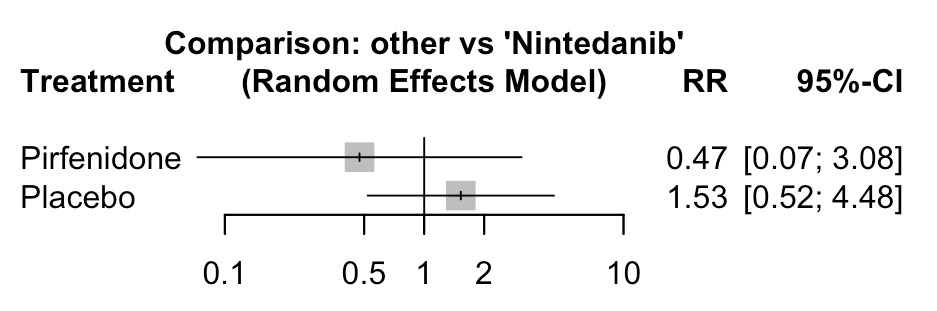
Exacerbation/hospitalization: Three trials (INPULSIS-1, INPULSIS-2, ASCEND) contributed exacerbation/hospitalization data. Pirfenidone decreased exacerbation risk when compared to placebo (RR 0.31; 95% CI 0.15–0.64; p = 0.002), whereas nintedanib did show reduced risk of exacerbations but this result did not reach statistical significance. (RR 0.64; 95% CI 0.39–1.06; p = 0.08). On indirect comparison, pirfenidone reduced the risk of exacerbations/hospitalizations but this result also did not achieve significance (RR 0.48; 95% CI 0.20–1.17; p = 0.11). Heterogeneity was substantial (I² = 78.5%, τ² = 0.47; Q p = 0.03) likely reflecting a difference in endpoint definitions.
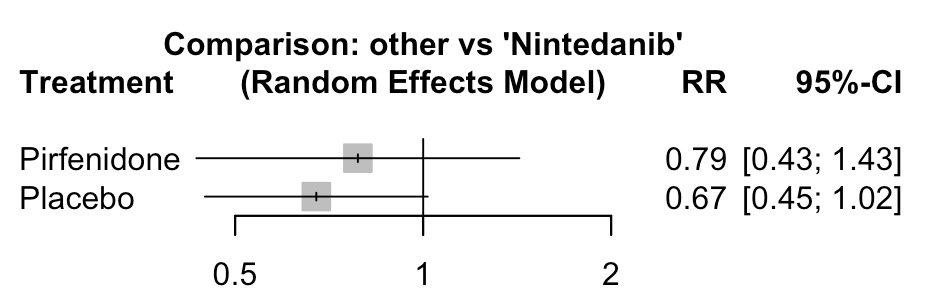
Treatment discontinuation: All four trials reported rates of discontinuation due to adverse effects. Nintedanib trended towards increased rates of discontinuation, but this was not statistically significant (RR 1.48; 95% CI 0.98–2.24; p = 0.06). In contrast pirfenidone’s rate of discontinuation was similar to placebo (RR 1.17; 95% CI 0.76–1.79; p = 0.48). Using indirect comparisons, pirfenidone was associated with a 21% lower risk of discontinuation when compared with nintedanib (RR 0.79; 95% CI 0.43–1.43; p = 0.43). Moderate heterogeneity was observed (I² = 45.5%, τ² = 0.04; Q p = 0.16).
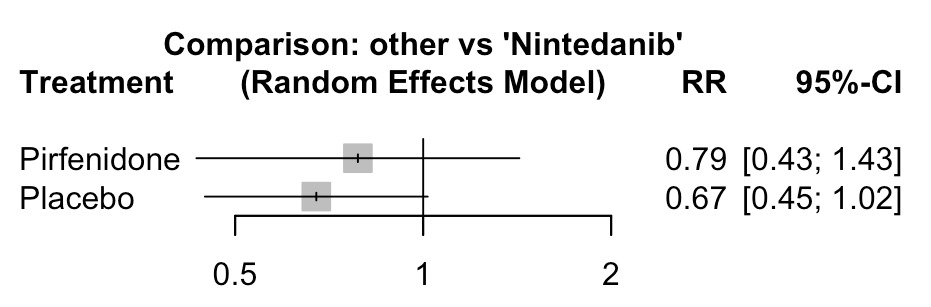
Figures 1-4 illustrate the key findings detailed above.
Reporting Biases
Reporting bias could not be formally assessed using funnel plots or regression-based methods because only four randomized controlled trials were available. As a result, the presence of small-study or publication bias cannot be excluded.
Certainty of Evidence
The certainty of evidence was evaluated for each outcome using GRADE methodology. For the outcome of a ≥10% decline in forced vital capacity (FVC), the certainty of evidence was rated as high, as all included trials demonstrated a low risk of bias, minimal heterogeneity, and direct comparisons between active treatment and placebo.
For all-cause mortality, the certainty of evidence was judged to be moderate. Although the included studies exhibited low risk of bias and consistent findings, estimates were imprecise, with confidence intervals crossing the line of no effect (risk ratio confidence intervals including 1.0), resulting in a one-level downgrade for imprecision.
The certainty of evidence for acute exacerbations or hospitalizations was rated as low. This assessment was downgraded by one level for imprecision due to wide confidence intervals and an additional level for substantial heterogeneity across studies (I² = 78%).
For treatment discontinuation due to adverse events, the certainty of evidence was considered moderate, with a one-level downgrade for imprecision, reflected by moderate heterogeneity (I² = 45%).
Overall, considering all outcomes collectively, the total body of evidence was judged to provide moderate certainty.
Discussion
Summary of Findings
In this systematic review and Bayesian network meta-analysis of phase III randomized controlled trials, both pirfenidone and nintedanib were associated with reduced risk of clinically significant lung function decline compared with placebo in adults with idiopathic pulmonary fibrosis. The indirect comparison suggested that pirfenidone may be more effective than nintedanib in reducing the decline in forced vital capacity of at least 10%. In contrast, no statistically significant between-drug differences were observed for mortality, acute exacerbations, or treatment discontinuation due to adverse events.
These findings are clinically relevant because direct comparative data between approved antifibrotic therapies remain unavailable, yet treatment selection is a common and practical challenge in the care of patients with IPF. The present analysis adds value by focusing specifically on phase III randomized trials, thereby restricting the evidence base to studies with more standardized patient selection, dosing, follow-up, and endpoint ascertainment than broader reviews that combine early-phase or observational data. This design choice was intended to strengthen internal validity and improve comparability across treatment nodes within the network.
The most robust finding of this analysis was the effect on forced vital capacity decline. In IPF, decline in forced vital capacity is a clinically meaningful surrogate of disease progression and has been widely used as a regulatory and trial endpoint. Both antifibrotic agents improved this outcome relative to placebo, supporting current treatment paradigms. The indirect estimate favoring pirfenidone is hypothesis-generating and may be important, but it should not be overstated. The absence of direct head-to-head randomized trials means that this apparent advantage depends on the assumptions of network meta-analysis, particularly transitivity and comparability across trials.
The lack of significant mortality differences is not surprising. Mortality events over approximately 1 year are relatively infrequent in trial populations, and available studies were not primarily powered to detect mortality differences between active treatments. Similarly, the nonsignificant findings for acute exacerbations and treatment discontinuation likely reflect limited power, event rarity, and potential variability in outcome definitions and reporting.
Strengths and Limitations
This network meta-analysis has strengths, including high internal validity from phase III randomized, placebo-controlled trials. It examined four outcomes: lung function decline, mortality, exacerbations, and treatment discontinuation. Robust statistical methods were used, including risk ratios, a frequentist random-effects model, heterogeneity analyses, and bias analyses. GRADE criteria provided an objective data quality assessment. Notably, this is the first study comparing outcomes of nintedanib and pirfenidone using data exclusively from RCTs.
Several limitations should be acknowledged. Most importantly, the comparison between pirfenidone and nintedanib is indirect because no head-to-head randomized trial was available. The network was small and star-shaped, limiting formal inconsistency assessment. The number of included studies was modest, reducing statistical power for less frequent outcomes such as mortality and acute exacerbations. Some outcomes may also have varied in definition across trial programs. In addition, if screening and extraction were performed by a single reviewer, that process may have increased the risk of selection or extraction error despite use of predefined criteria. Finally, exclusion of non-English reports and unpublished data may have introduced reporting bias, although the pivotal phase III IPF literature is relatively well characterized.
Implications
This study’s findings support the use of antifibrotics in the management of IPF and demonstrate that both nintedanib and pirfenidone significantly slow disease progression in IPF. However, this analysis demonstrates that pirfenidone has additional benefits in the preservation of lung function, and potential exacerbation reduction and has an improved tolerability profile when compared to nintedanib. Clinicians should consider these results when entering shared decision-making conversations with their patients, especially those who are at a greater risk for lung-function decline and drug discontinuation.
Future Research Directions
To validate the findings of this analysis, high-quality, adequately powered direct head-head trials are urgently required, ideally with prespecified mortality and acute exacerbation endpoints with follow-up times beyond 1 year. In addition, future network meta-analyses should be conducted to further clarify the impact that baseline characteristics (FVC, age, sex, comorbidities) have on similar outcomes. Furthermore, future studies should consider using real-world registry data to measure the effectiveness and safety of antifibrotic therapy in broader, more heterogenous populations. Finally, future studies should consider exploring combination antifibrotic therapies due to complementary mechanisms of action.
Conclusions
In this systematic review and Bayesian network meta-analysis of phase III randomized controlled trials involving 4 trials and 1,931 patients, both pirfenidone and nintedanib significantly reduced the risk of FVC decline when compared with placebo. However, pirfenidone demonstrated more-effective lung function preservation while simultaneously having a better tolerability profile when compared to nintedanib. Furthermore, pirfenidone trended towards superiority in exacerbation reduction when compared to nintedanib. However, neither agent showed substantial mortality reduction. In summary, this analysis provides the best evidence to date to inform antifibrotic selection in IPF while simultaneously demonstrating the need for further research and direct comparative trials.
Funding
This research received no external funding.
Conflicts of Interest
There are no conflicts of interest to declare.