Highlights of the Study
-
First study in Kuwait evaluating perioperative and postoperative analgesic practices in elective bariatric surgeries.
-
A structured educational intervention was delivered by a PharmD trainee.
-
Post-intervention analysis showed reduced opioid use and discontinuation of outdated agents.
-
Another outcome was the implementation of a pain assessment tool.
-
Findings underscore the importance of clinical pharmacists and trainees in supporting opioid stewardship.
1. Introduction
Obesity has emerged as one of the most challenging global public health issues of the 21st century. Recent advancements in obesity treatment emphasize a comprehensive, individualized approach that integrates lifestyle modifications, pharmacotherapy, and, when appropriate, surgical interventions. Metabolic and bariatric procedures can lead to significant and sustained weight loss, improving or resolving comorbidities.1–4
Kuwait leads globally in obesity rates, with nearly 40% of adults classified as obese, and is the Arbian Gulf country with the highest number of metabolic and bariatric procedures per national population.5 Despite better understanding of nociception and progress in pharmacology, up to 41% of patients suffer from severe pain within the first two days following their surgery.6 Inadequate postoperative pain management may result in serious complications, such as decreased intestinal motility, slowed wound healing, cardiac ischemia, immunologic alterations, pulmonary complications, as well as a higher risk of thrombosis due to immobility.7 Multimodal approach of analgesics means using two or more pain medications with different mechanisms of actions. The ultimate goals of such multimodal analgesia approach in patients undergoing metabolic and bariatric surgery are to enhance pain relief, minimize opioid use and the risk of opioid-related respiratory complications, and facilitate early recovery and mobility.8
This is the first study in Kuwait and in the Arabian Gulf Region -up to our best knowledge- that reviews and assesses the use of analgesics in elective metabolic and bariatric surgeries, including the choice and types of medications used, dosage regimen, and duration of use in the peri and postoperative period in a single center in Kuwait. Furthermore, this study aims at assessing the influence of a lecture concerning the recommended practice of analgesics prescribing during such surgeries delivered by a PharmD trainee to surgeons, anesthesiologists, and nurses.
2. Subjects and Methods
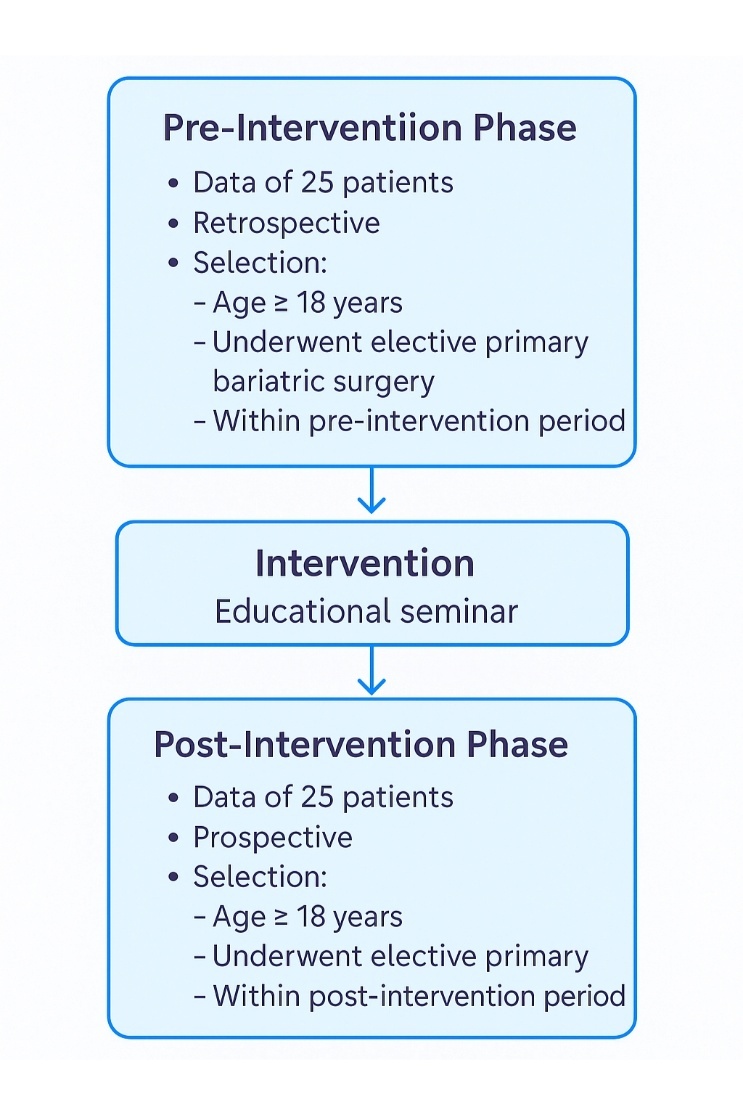
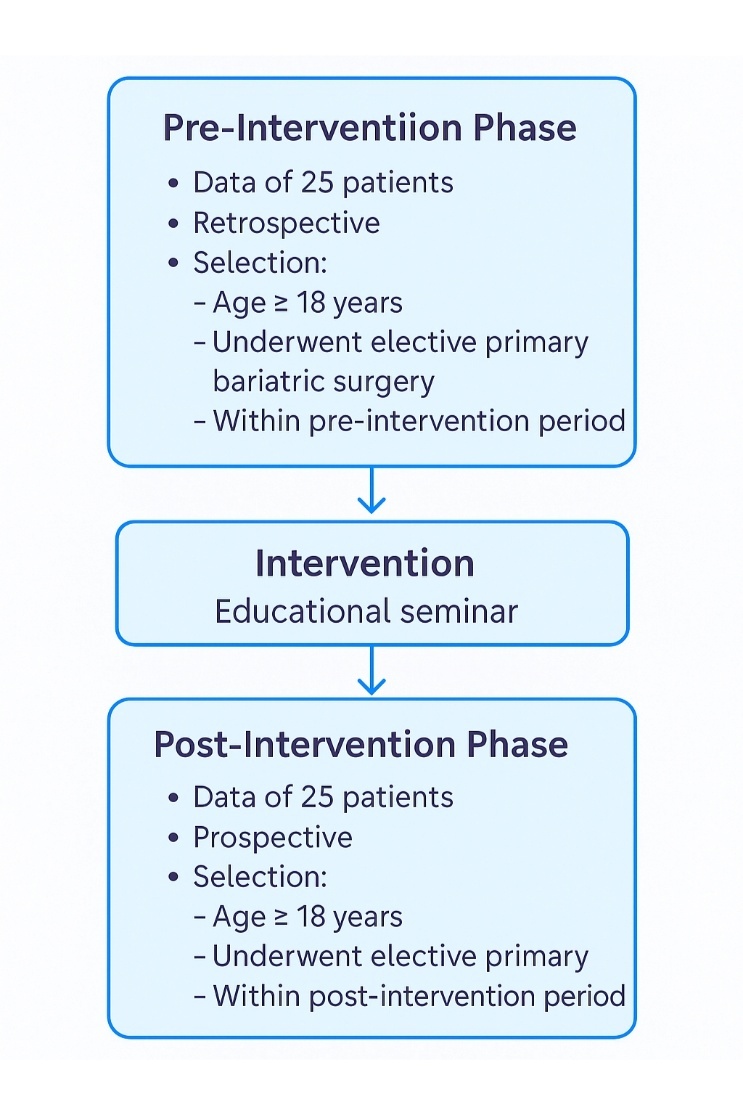
Ethical approval was granted by Kuwait University Health Sciences Centre Ethics Committee for student research before starting this study. Data from patients who underwent elective laparoscopic bariatric surgery at a governmental hospital, Al Amiri hospital, from September 11, 2022 to January 5th, 2023, were evaluated retrospectively. The study inclusion criteria involved any patient aged 18 years and above who had elective primary metabolic and bariatric surgery during the assigned study period.
Patients’ demographics, including age, gender, and nationality, were recorded. Other information related to past medical and medication history, and data regarding smoking status, allergies, and Body Mass Index (BMI). Based on BMI, obesity was divided into three categories: obesity class I (BMI 30-34.9 Kg/m2), obesity class II (BMI 35-39.9 Kg/m2), and obesity class III, known as morbid obesity (BMI ≥ 40 Kg/m2) (Centers for Disease Control and Prevention, 2022). Elective metabolic and bariatric surgeries to be observed in this study were sleeve gastrectomy, roux en Y gastric bypass, one anastomosis gastric bypass, gastric-band, and biliopancreatic diversion with duodenal switch. The duration of anesthesia and surgery was defined and recorded as the interval from anesthesia administration until surgery completion and patients’ discharge to the recovery room.
An educational seminar in line with the best practices of analgesic use in perioperative and postoperative periods was developed and delivered by a PharmD trainee, this is referred to as the intervention in this study. The intervention targeted healthcare providers at Amiri hospital (physicians from surgical, anesthesia and nursing departments). It was delivered in November 2022 after the initial data collection and analysis of pre-interventional period was completed (September to October 2022). Figure 1 demonstrates the study design.
In the data collection form, medications were categorized into three sections: pre-operative, intra-operative, and post-operation medication. Medications were general, local and inhaler anesthetics, analgesics, sedatives, muscle relaxants, and other classes. It should be noted that intra-operative analgesia was administered depending on each anesthesiologist’s clinical judgment and preference. Similar to analgesia, the choice of the anesthesia used to initiate the surgeries depended on the anesthesiologists’ judgment due to the lack of current protocol to follow. Additionally, data regarding local anesthesia were challenging to retrieve since the information was documented in different sheets and computer systems. Data analysis for this study was performed and completed using Microsoft Excel software.
3. Results
Data of a total of 50 patients were recruited in this study from September 2022 to January 2023. Twenty-five patients’ data were reviewed in the pre-educational period. As part of a non-direct patient care educational initiative, also referred to here in this study as “the intervention”, a PharmD trainee delivered a one-hour lecture to 25 healthcare professionals, including surgeons, anesthesiologists, and nurses, focusing on optimizing analgesic prescribing practices in elective metabolic and bariatric surgeries. The session was supported by a structured PowerPoint presentation summarizing findings from a baseline pilot observational study conducted at Amiri Hospital, and a concise clinical education material (reference sheet) outlining perioperative analgesic options and dosing strategies. The lecture emphasized the importance of implementing a multimodal analgesic approach, minimizing reliance on opioids, and individualizing therapy to improve postoperative outcomes and patient safety.
Another 25 patients’ data were collected then as the post-intervention/post-educational sample and the influence of the educational seminar on analgesic practice was assessed. Table 1 summarizes key demographic descriptors for all patients included in this study from both pre-intervention and post-intervention groups.
Allergies were seen in 24% (n= 6) of the patients in pre-intervention, of which medication allergy accounted for 8% (n=2). One patient had a penicillin allergy, and the other patient was allergic to cetirizine. The percentage of allergy seen in the post-intervention period is 8% (n=2), of which one patient had morphine-related drugs allergy, and the other had streptomycin allergy. However, 8% (n= 4) of the enrolled patients did not have an allergy status, refer to Table 1. More than half of the patients in each group had at least one comorbidity (60% of the patients in the pre-intervention period and 64% in the post-intervention period). These comorbidities were mainly hypertension (HTN), type 2 diabetes mellitus (T2DM), gastroesophageal reflux disease (GERD), hypothyroidism, obstructive sleep apnea (OSA), and to a lesser extent, dyslipidemia, fatty liver disease, asthma, thrombotic events (stroke and deep vein thrombosis), and type 1 diabetes mellitus. Medication history was documented in 52% (n= 13) of the patients’ medical records in the pre-intervention period and 56% (n= 14) in the post-intervention period. Medications documented were antihypertensive agents (Valsartan, Hydrochlorothiazide, Bisoprolol), low-dose Aspirin, antihyperglycemic agents (Insulin and Metformin), proton-pump inhibitors (PPI- Omeprazole and Esomeprazole), thyroid replacement therapy (levothyroxine), bronchodilators (Salbutamol, Albuterol, Tiotropium bromide, and Formoterol format) and Inhaler corticosteroids (Fluticasone propionate) for asthma, and statins (Rosuvastatin), refer to Table 1. Surgery duration performed in both pre-intervention and post-intervention periods was documented in 88% (n= 44), which ranged approximately from half an hour to almost five hours in length. Table 2 below compares between the non-pain medications given to patients from both groups, pre- and post- the educational intervention groups.
Intravenous antibiotic prophylaxis was administered routinely to most patients in pre-intervention and post-intervention periods (88% [n= 22], 96% [n= 24], respectively) on the day of the procedure. Pre-operative antibiotic prophylaxis includes one of the following: clindamycin (Dalacin C®), ceftriaxone, cefotaxime (Claforan®), cefuroxime (Zinacef®), and cefazolin, refer to Table 2. After that, patients received general anesthesia in parallel with a variety of intra-operative medications to initiate laparoscopic bariatric surgery with the patient in the standard supine position. The general anesthesia agents used include propofol, fentanyl, remifentanil, ketamine, and lidocaine (Table 2). There was no established anesthesia protocol or policy to follow. In all patients (100%, n= 50), induction of general anesthesia was done intravenously, and maintenance was done by inhalation anesthesia. However, at least one patient (4%) in the pre-intervention period and two patients (8%) recruited in the post-intervention period received lidocaine 1%.
As for the multimodal intra-operative analgesia, it consists of paracetamol, with either a non-steroidal anti-inflammatory drug (NSAID) or opioid, or both. This multimodal intra-operative analgesia was given to 92% (n= 46) of the assigned patients. In the pre-intervention period About 60% (n= 15) received Paracetamol + Parecoxib + Oxycodone; 12% (n= 3) received Paracetamol + Parecoxib + Oxycodone + Tramadol; 4% (n= 1) received Paracetamol + Parecoxib + Oxycodone +Tramadol + Meperidine; 8% (n= 2) received Paracetamol + Parecoxib + Morphine; 4% (n= 1) Paracetamol + Oxycodone; 4% (n= 1) received Paracetamol + Tramadol; 4% (n= 1) received Paracetamol + ketorolac; and 4% (n= 1) received Tramadol + Morphine, refer to Table 3. In comparison, 44% (n= 11) of patients assigned in the post-educational period received Paracetamol + Parecoxib + Oxycodone; 24% (n= 6) received Paracetamol + Parecoxib + Oxycodone + Tramadol; 8% (n= 2) received Paracetamol + Parecoxib + Morphine; 12% (n= 3) received Paracetamol + Morphine; 4% received Paracetamol + Oxycodone + Tramadol; 4% (n= 1) received Tramadol + Morphine, and 4% (n= 1) received Paracetamol only (Table 3). There is no difference between the population who received multimodal analgesia in the pre-education and post-education periods (92%, n= 23 in both periods).
In addition, midazolam (Dormicum®) was used as a sedative. Muscle Relaxants were also included in the intra-operative medications. They include rocuronium bromide (Esmeron®), cisatracurium besilate (Nimbex®), sugammadex, and suxamethonium chloride (Scoline®). Other intraoperative medications are dexamethasone, hydrocortisone, reverse neostigmine, ephedrine, phenylephedrine, and atropine.
Patients in the Post-Anesthesia Care Unit (PACU) also received multimodal analgesia. Only 28% (n= 7) of the pre-intervention population and 24% (n= 6) received multimodal analgesia during their PACU stay. Whether the analgesics were received or ordered is not documented in around 34% (n= 17) of the total patients’ records. Analgesics were administered 0–2 hours after admission to the PACU. Analgesic agents used include paracetamol (Perfalgan®), oxycodone (Oxynorm®), tramadol (Tramal®), morphine, and meperidine (Pethidine®) (Table 3). Table 4 summarizes the total number of each prescribed analgesic during metabolic and bariatric surgeries involved in this study.
Multimodal analgesia has also been provided for in-ward. It was administered to 64% (n= 16) of patients enrolled in the pre-educational period and 32% (n= 8) in the post-intervention population (Table 3). Pain medications that were given intravenously to the patients in the surgical ward on as needed basis were paracetamol 1g every 6–8 hours (Perfalgan®), tramadol 100 mg every 8 hours (Tramal®), and parecoxib 40 mg twice daily (Dynastat®). According to the Lexicomp database, tramadol 50 mg–100 mg could be given orally every 4 to 6 hours as needed. In-ward analgesic re-dosing occurs three to four hours after the last dose in the PACU. None of the patients were taking opioids chronically prior to their procedure. Patient-controlled analgesia pumps, PCA, were not used in any of the patients during their stay in the surgical ward. Pain assessment was performed in 32% (n= 8) of the patients who were reviewed after the educational seminar. Out of these, a numerical pain scale was used in three patients to evaluate their pain level.
4. Discussion
Several similar studies were conducted worldwide to assess and optimize the prescribing practice of analgesics during metabolic and bariatric surgeries and the recovery phase afterwards. Commonly the main goal of such studies is to encourage more opioid sparing regimens to help control/prevent opioid dependence.9–12 The multimodal analgesic approach provides better efficacy and fewer complications after the surgeries.8,13 Multimodal analgesia is composed of the use of multiple analgesics acting at the same time through various mechanisms in order to create efficient synergistic analgesia with lesser side effects. About 92% of patients in this study received multimodal intraoperative analgesia. There was no difference between the number of patients who received a multimodal analgesic approach in both periods of the study (n= 23 in each period). The majority of the patients received Paracetamol + Parecoxib + Oxycodone as intraoperative multimodal analgesia in pre-intervention and post-intervention periods (60%, and 40%, respectively). There was a drop in the percentage of patients who received multimodal analgesia in the PACU after the educational period (multimodal analgesia in 28% (n=7) of the pre-intervention population Vs. multimodal analgesia use in 20% (n= 5) of the post-intervention population). Oxycodone monotherapy was the most medication administered in the PACU in pre-intervention and post-intervention patients (20%, and 16%, respectively). The re-dosing in the PACU occurs 3.5 hours after the administration of the initial dose in the operating room, which is convenient with the duration of action of the medication. Although it does not show significant safety or efficacy, meperidine was administered to 8% (n= 2) of the patients in the pre-intervention period and to 4% (n= 1) of the patients in the post-intervention period.14 The choice of each analgesic was not explained in the medical record, and the choice of the medication was based on the anesthesiologists and surgeons’ judgment.
Because of the ongoing opioid crisis, healthcare providers must re-evaluate their practice in the utilization of opioids in order to lower patient dosages while still providing effective pain management. At the beginning of the study, there was a gap between the number of analgesic medications, including opioids, prescribed following metabolic and bariatric surgery and the experienced pain level by patients in the surgical ward, as there was no pain scale to assess the level of pain experienced by the patients. This issue was highlighted during the educational seminar. The PharmD Trainee addressed the need for a validated pain intensity assessment scale, for example, the Numeric Rating Scale, Verbal Rating Scale, and Visual Analogue Scales. The International Association for the Study of Pain (IASP) defines pain as “an unpleasant sensory and emotional experience” associated with actual or potential tissue damage, or described in terms of such damage.15
Elements of postoperative pain assessment are described in.16 These elements are quality of pain, onset and pattern, location, quality of pain, intensity, aggravating and relieving factors, previous treatment, effect, and barriers to pain assessment. In this study, the use of local anesthesia was either minimal in practice or poorly documented, highlighting the need to engage surgeons in addressing this issue.
Fortunately, pain assessment was conducted in 32% (n= 8) of the patients who were reviewed after the educational seminar. About 16% (n= 4) of the assessed patients experienced mild to moderate pain and received multimodal analgesia as needed to manage their symptoms. The remaining 8% (n= 2) experienced pain and received only Paracetamol 1 g every 6-8 hours as needed. No pain was experienced in around 8% (n= 2) of those who were assessed. In-ward multimodal analgesia was administered to 64% (n= 16) of patients recruited in the pre-education period, whereas administered to 32% (n= 8) in the post-intervention population, of which 16% (n= 4) had pain assessment.
When compared to published work, this study is consistent with global trends in using paracetamol as a baseline non-opioid analgesic due to its favorable safety profile, especially in obese populations where liver metabolism is critical.8,13 It aligns also with the encouraged use of selective COX-2 inhibitors -rather than non-selective- for safety and efficacy purposes, mainly reducing the risk of gastrointestinal side effects.13 Opioid use in this study was most commonly in combination rather than monotherapy in agreement with global recommendations.10,12 The educational intervention resulted in a slight reduction in opioid prescription, unlike similar reported intervention that resulted in a significant reduction in opioid use up to 50%.8 This reflects good practice of analgesic prescription in the title facility. Multimodal analgesia was used to a lesser extent in postoperative settings (PACU and in-Ward) in this case post intervention when compared to global settings.8,10 This can be attributed to the use of pain assessment tool that showed reduced need for stronger pain relief, especially that 100% of monotherapy prescribed for inward patients was nonopioid analgesics. Tan and colleagues conducted a similar intervention and assessment where they found that implementing a standardized pain control regimen and an educational program (for patients have significantly reduced inpatient opioid use in patients undergoing metabolic and bariatric surgery,8 while in this research the intervention was for healthcare professionals).The current study is limited by a short period (September 2022 to January 2023) and a small sample size of patients (n= 50); however, the study included all the patients undergoing metabolic and bariatric surgeries during the assigned time frame. The complexity of data retrieval was influenced by multiple factors, including inconsistencies in medical record documentation and the transition to electronic medical records, as the hospital was undergoing digital transformation during the study period. Further studies should be conducted and should focus on the relationship between provided analgesia regimen and pain levels in metabolic and bariatric surgery patients.
The findings of this study highlight several areas for improvement in the postoperative pain management. Routine use of validated pain assessment tools—such as the Numerical Rating Scale (NRS) or Visual Analog Scale (VAS)—should be implemented at all postoperative stages to ensure consistent evaluation. Integration of these scores into electronic health records is essential to support reliable documentation and informed clinical decision-making. The development of standardized, evidence-based multimodal analgesia protocols tailored to metabolic and bariatric patients is strongly recommended. These protocols should provide clear guidance on the judicious use of NSAIDs and opioid-sparing strategies, and the inclusion of non-opioid adjuvants. The study also underscores the need to educate surgical teams on the analgesic benefits of local anesthetics, alongside implementing standardized documentation practices to monitor their intraoperative use. Continuity of multimodal analgesia from the operating room to the PACU and inpatient wards is critical, with pain management adjusted according to individual patient-reported scores. Additionally, outdated agents such as meperidine should be omitted from practice. The involvement of clinical pharmacists in perioperative care, supported by PharmD trainees, may further enhance pain control and interdisciplinary collaboration. Finally, improving digital integration, documentation quality, and continuous professional education are key strategies to ensure sustainable advancements in analgesic practice.
5. Conclusions
This study identifies key areas to improve postoperative pain management in metabolic and bariatric surgery in Kuwait, including routine use of validated pain assessment tools, integration into electronic records, and the implementation of standardized multimodal analgesia protocols with opioid-sparing strategies and non-opioid adjuvants. It also emphasizes the importance of surgeon education on local anesthetics, enhanced documentation, interdisciplinary collaboration, and ongoing digital and professional development efforts to ensure sustained improvements.
Statement of Ethics
This study protocol was reviewed and approved by Kuwait University Health Sciences Centre Ethics Committee for student research, approval number 1264, granted on 14 June 2022. Consent forms were not collected due to the retrospective nature of the study.
Conflict of Interest Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding Sources
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Contributions
T.B. and A.A. conceived the study. G.A., K.G., and R.A. collected the data. T.B. performed the statistical analyses. T.B. and A.A. cross checked the data. T.B. drafted the manuscript, and all authors contributed substantially to its revision.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgements
None.