1. Introduction
Laparoscopic cholecystectomy is the standard treatment for symptomatic cholelithiasis and one of the most commonly performed operations worldwide.1 Gallbladder perforation with spillage of bile and gallstones is a recognized intraoperative occurrence, especially in difficult dissections.1,2 Although efforts are made to retrieve spilled stones, some are inevitably retained. In most cases, these remain clinically silent.2
When complications occur, they are often delayed and difficult to attribute to the initial surgery.2,3 Reported sequelae include intra-abdominal abscesses, inflammatory masses, fistula formation, and bowel obstruction.1–4 These cases are frequently marked by recurrent hospitalizations and interventions before diagnosis. Abscess formation is the most common presentation and is typically managed with antibiotics and percutaneous drainage.1
However, retained stones can prevent complete resolution and lead to recurrence.1,5 This is particularly challenging in anatomically difficult regions such as the posterior hepatic space.3 In these cases, definitive management often requires operative intervention.5 We present a case of recurrent posterior hepatic abscesses due to retained gallstones requiring robot-assisted retrieval using indocyanine green localization.
2. Case Presentation
A 75-year-old male with a history of hypertension, hyperlipidemia, chronic obstructive pulmonary disease, gastroesophageal reflux disease, diverticular disease, prior gastrointestinal bleeding, cholelithiasis, and choledocholithiasis was evaluated for recurrent intra-abdominal infections following laparoscopic cholecystectomy. He had documented allergies to chlorhexidine gluconate and sulfonamides. In June 2023, he underwent ERCP with metal biliary stent placement for choledocholithiasis, followed by laparoscopic cholecystectomy in July 2023. The operative report from this procedure detailed extensive acute and chronic inflammation with dense adhesions involving the gallbladder and omentum. During dissection, the fundus of the gallbladder was perforated, releasing pale yellow, sludgy fluid, and the gallbladder was noted to be packed with stones. The triangle of safety and cystic duct could not be identified due to severe inflammation, and a subtotal dissection was required. Intraoperative gallstone spillage was not explicitly documented, but these operative findings made stone spillage highly likely.
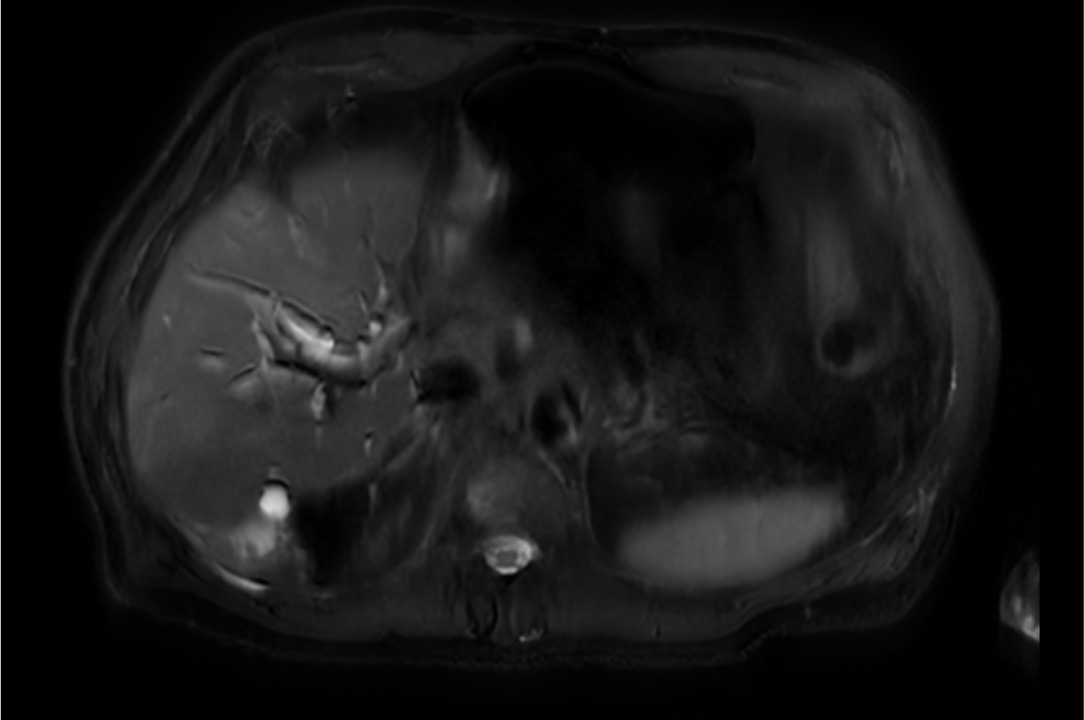
His postoperative course was complicated by a gallbladder fossa abscess requiring percutaneous drainage, and the biliary stent was removed in September 2023. He remained stable until April 2025, when he presented with right upper quadrant pain, fever, nausea, vomiting, and altered mental status. He was hypotensive and febrile, with blood cultures growing Escherichia coli. Imaging demonstrated pneumobilia and inflammation adjacent to retained gallstones along the posterior liver. He improved with intravenous antibiotics and was discharged on suppressive therapy.
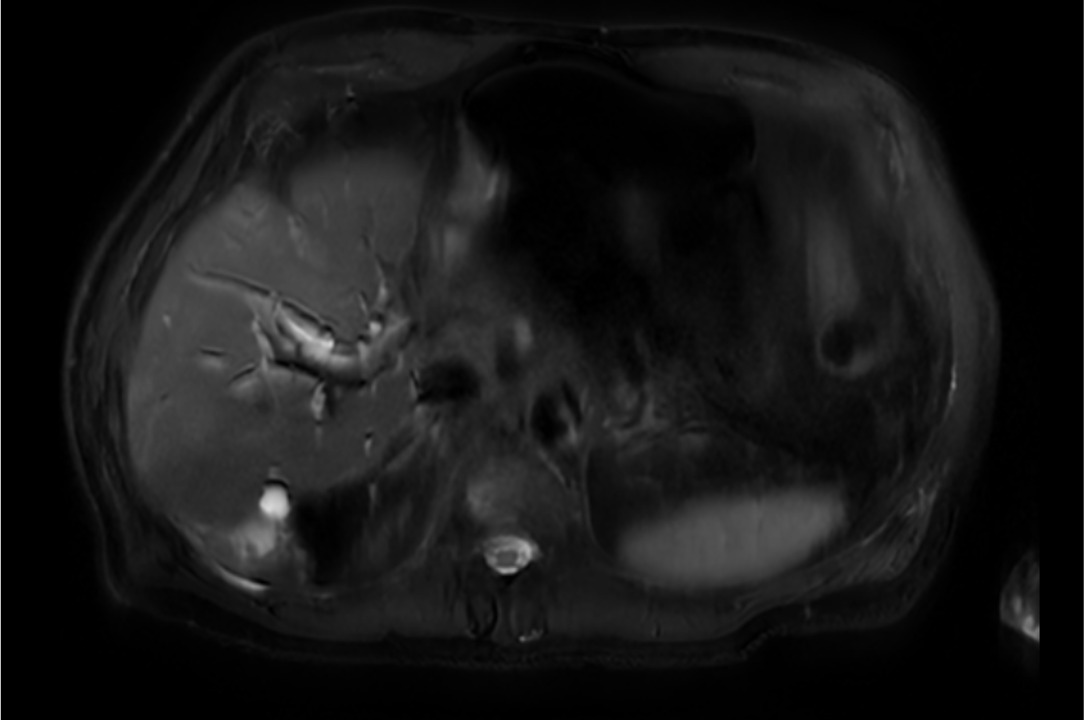
Within ten days, he was readmitted with recurrent fever and altered mental status. Imaging suggested ascending cholangitis and a perihepatic fluid collection. He underwent ERCP with sludge removal and stent placement, followed by CT-guided drainage. Cultures revealed polymicrobial infection, including multidrug-resistant Klebsiella pneumoniae. Recurrent infections persisted despite repeated hospitalizations and antibiotics. In October and November 2025, imaging continued to show persistent collections and retained stones despite drainage and intravenous ertapenem, prompting operative management.
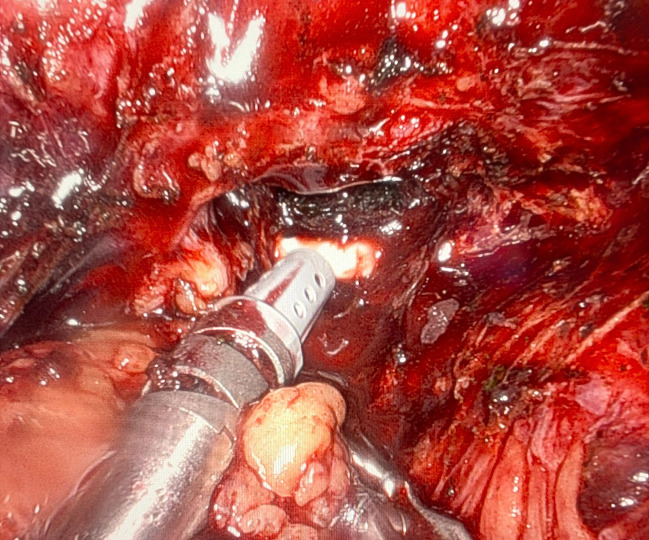
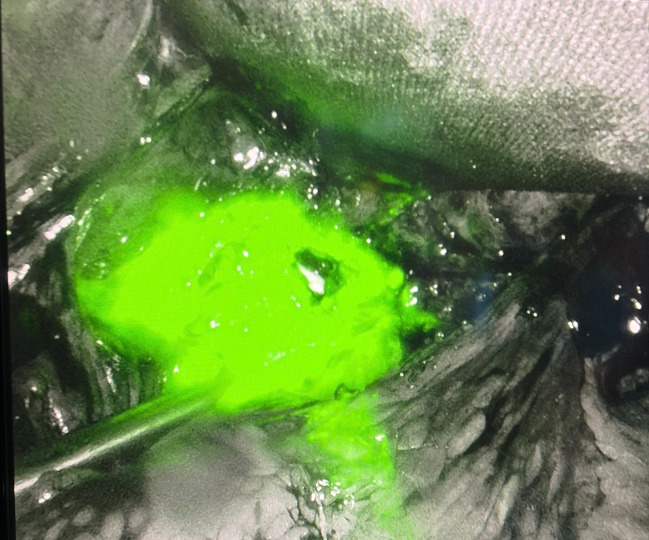
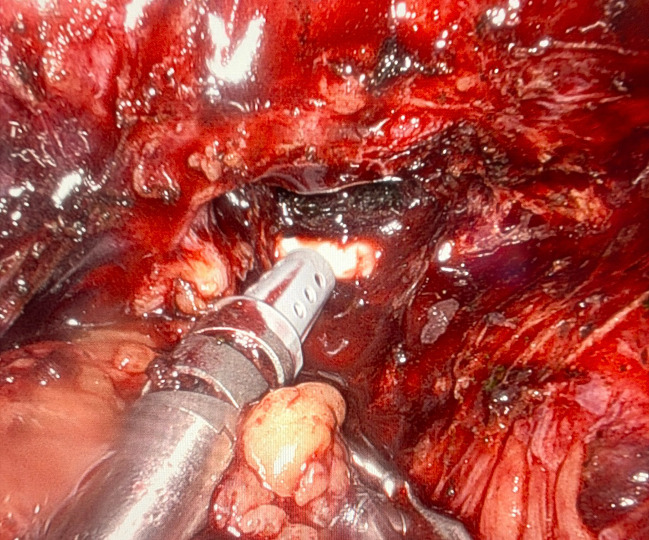
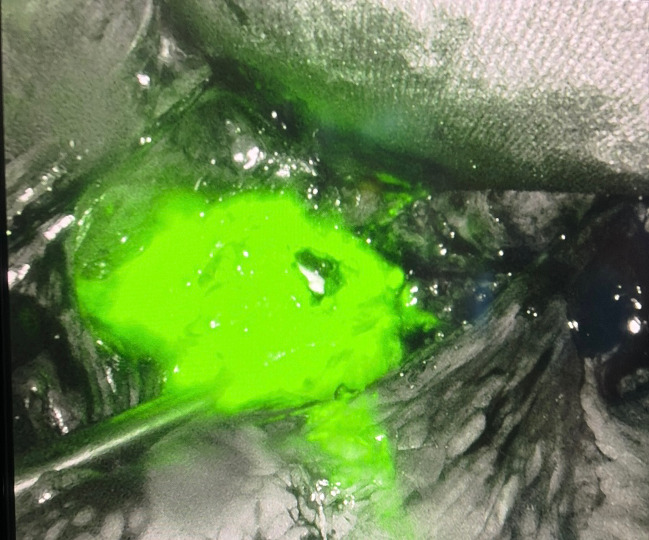
He underwent a robot-assisted exploratory surgery lasting a total of 35 minutes. Pneumoperitoneum was established using the Hasson technique, and robotic ports were placed in the right abdomen. The liver was elevated to expose the posterior hepatic surface, where dense inflammatory changes were encountered. Indocyanine green was injected through the existing percutaneous drain, allowing fluorescence-guided localization of the abscess cavity using near-infrared imaging. The cavity was opened, and multiple retained gallstones were identified and removed using a specimen retrieval bag. The aggregate of gallstones collected within the retrieval bag was measured to be 2.5 x 0.5 x 0.3 cm. The cavity was irrigated, and the existing drain was left in place. It was estimated that the patient had no blood loss during the procedure. The patient tolerated the procedure well and was discharged on postoperative day two with a two-week course of ertapenem. No additional antibiotic therapy was required. He subsequently underwent ERCP with biliary stent removal eight weeks later without any complications.
3. Discussion
This case highlights a pattern increasingly recognized in patients with retained gallstones: recurrent infections without definitive source control.1,2,5 Although each intervention was appropriate, none addressed the underlying issue. Retained stones acted as a persistent nidus for infection, resulting in temporary improvement followed by recurrence. This reinforces a key principle: without removal of the offending stone, long-term resolution is unlikely.
Initial management of intra-abdominal abscesses typically includes antibiotics and percutaneous drainage, which remain appropriate first-line strategies.1 However, when imaging demonstrates retained gallstones within a persistent or recurrent collection, these measures alone are often insufficient.1,2,5 Continued reliance on nonoperative management may delay definitive treatment and prolong morbidity, particularly in patients with repeated hospitalizations. Earlier consideration of operative intervention in such cases may shorten the clinical course.
Previous reports have described minimally invasive and combined interventional approaches for the retrieval of retained gallstones in anatomically challenging locations. Operative management of retained gallstones in difficult locations, such as the posterior hepatic space, has traditionally required open exploration, which carries increased morbidity in older patients with comorbidities.1 Conventional laparoscopic approaches offer the advantages of minimally invasive surgery but may be limited by dense adhesions, chronic inflammation, and difficulty localizing retained stones.3,5 More recently, Mushtaq et al. described a combined interventional radiology and surgical cut-down approach in which preoperative image-guided localization facilitated targeted retrieval of retained gallstones.5 This report similarly emphasizes the importance of accurate localization when operative access is limited by inflammation and distorted anatomy. In contrast, the technique described in this case used indocyanine green injected through an existing percutaneous drain to provide real-time fluorescence-guided visualization of the abscess cavity throughout the dissection. This dynamic approach allowed continuous delineation of the target and offered greater intraoperative flexibility than static localization techniques while preserving the benefits of a fully minimally invasive robotic approach.5
This technique represented a practical extension of indocyanine green’s established role in hepatobiliary surgery.5 While commonly used to identify biliary anatomy or assess perfusion, its application for abscess localization via a percutaneous drain is not widely reported. The robotic platform further enhanced this approach by improving visualization and instrument control in a confined anatomical space, facilitating precise dissection along the posterior liver and avoiding open surgery.5
4. Conclusion
Overall, retained gallstones should be considered in patients with recurrent intra-abdominal infections following laparoscopic cholecystectomy. When infections persist despite appropriate medical and interventional management, definitive stone removal is necessary for source control. This case demonstrates that a robot-assisted approach combined with indocyanine green localization is a feasible and effective minimally invasive strategy for managing retained gallstones in challenging anatomical locations and may improve outcomes in similar cases.
5. Declarations
5.1. Ethics approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images
5.2. Availability of data and material
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
5.3. Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
5.4. Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
5.5. Author’s contributions
PL performed the literature review, drafted the manuscript, and organized the clinical data and figures. JS and AK conceived the report, provided clinical oversight, and critically revised the manuscript for important intellectual content. All authors reviewed and approved the final manuscript and agree to be accountable for all aspects of the work.
5.6. Acknowledgements
None