Introduction
Genitourinary tuberculosis (GUTB) represents one of the most frequent forms of extrapulmonary tuberculosis and usually occurs secondary to hematogenous dissemination from a primary pulmonary focus. It can involve the kidneys, ureters, bladder, and genital organs, leading to progressive structural damage and functional impairment.1
Ureteric involvement is common, particularly affecting the distal ureter, and is characterized by chronic inflammation, fibrosis, and stricture formation. Radiological findings such as beading, corkscrew appearance, and pipe-stem ureter reflect alternating segments of fibrosis and dilatation.2 Persistent obstruction may result in hydroureteronephrosis, vesicoureteral reflux, and eventual renal function loss if not managed appropriately.
Upper ureteric strictures following GUTB are less common and present unique surgical challenges due to dense fibrosis and poor vascularity. Buccal mucosa graft (BMG) ureteroplasty has recently emerged as a viable reconstructive option for long-segment and complex ureteric strictures. We present a case of post-tubercular upper ureteric stricture successfully managed with open BMG ureteroplasty.
Case Presentation
A 28-year-old male with a known history of genitourinary tuberculosis presented with intermittent right flank pain and dysuria. He had completed six months of antitubercular therapy and previously underwent right double-J (DJ) stenting for right-sided hydroureteronephrosis. The DJ stent was exchanged at two and four months and subsequently removed.
Following stent removal, the patient developed recurrent symptoms suggestive of ureteric obstruction. Physical examination was unremarkable, and there were no constitutional symptoms.
Investigations
Baseline laboratory investigations, including complete blood count, liver function tests, and renal function tests, were within normal limits. Urinalysis revealed sterile pyuria.
Radiological and endoscopic evaluation included:
-
Ultrasonography: Right hydroureteronephrosis was observed.
-
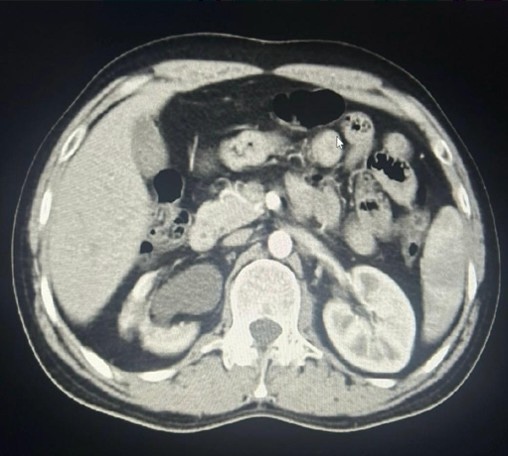
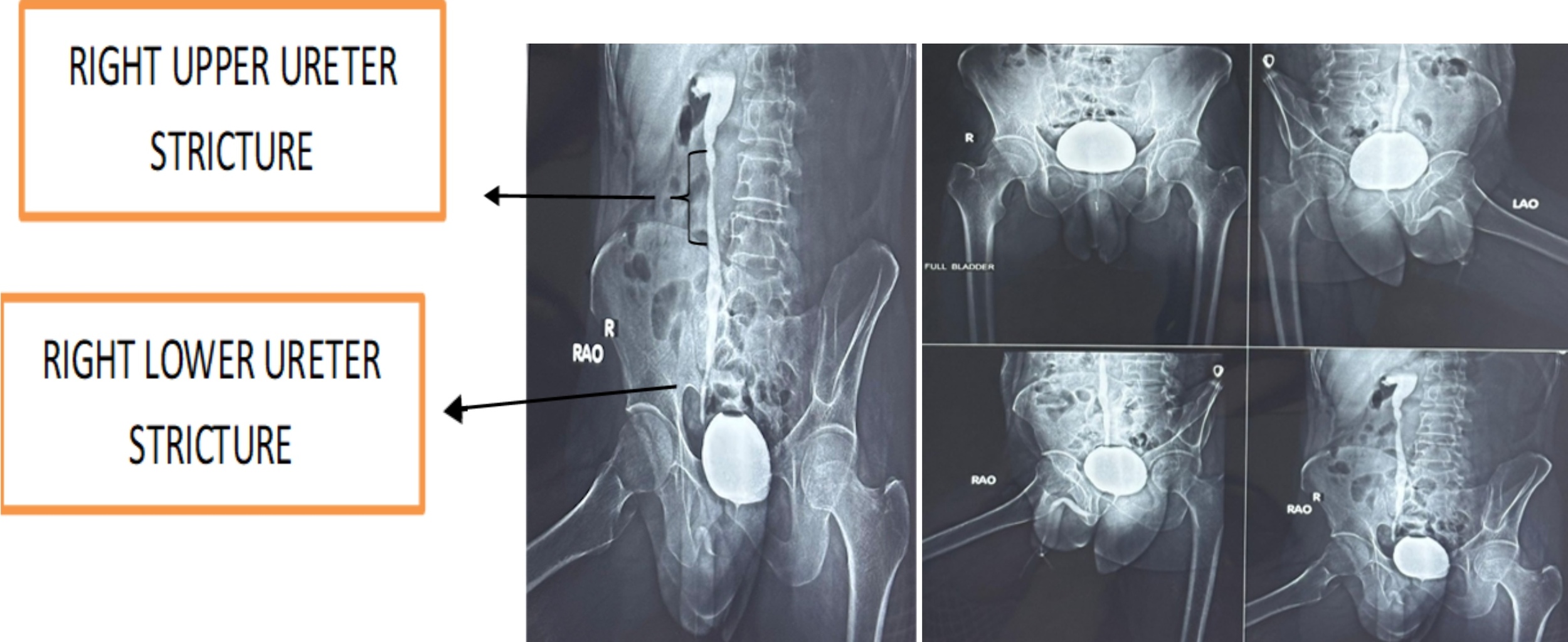
Contrast-enhanced CT abdomen and pelvis: Right hydroureteronephrosis with architectural distortion and ureteric strictures involving the upper and lower thirds (Figure 1A)

-
Preoperative CT urography demonstrated segmental circumferential urothelial thickening involving the proximal and distal right ureter with luminal narrowing and reduced contrast opacification, associated with upstream pelvicalyceal dilatation. The right kidney showed significant parenchymal volume loss with cortical irregularity and small calcifications, along with a lower pole cortical cyst. Findings were suggestive of chronic inflammatory pathology, likely genitourinary tuberculosis, with preserved function in the contralateral kidney (Figure1B).
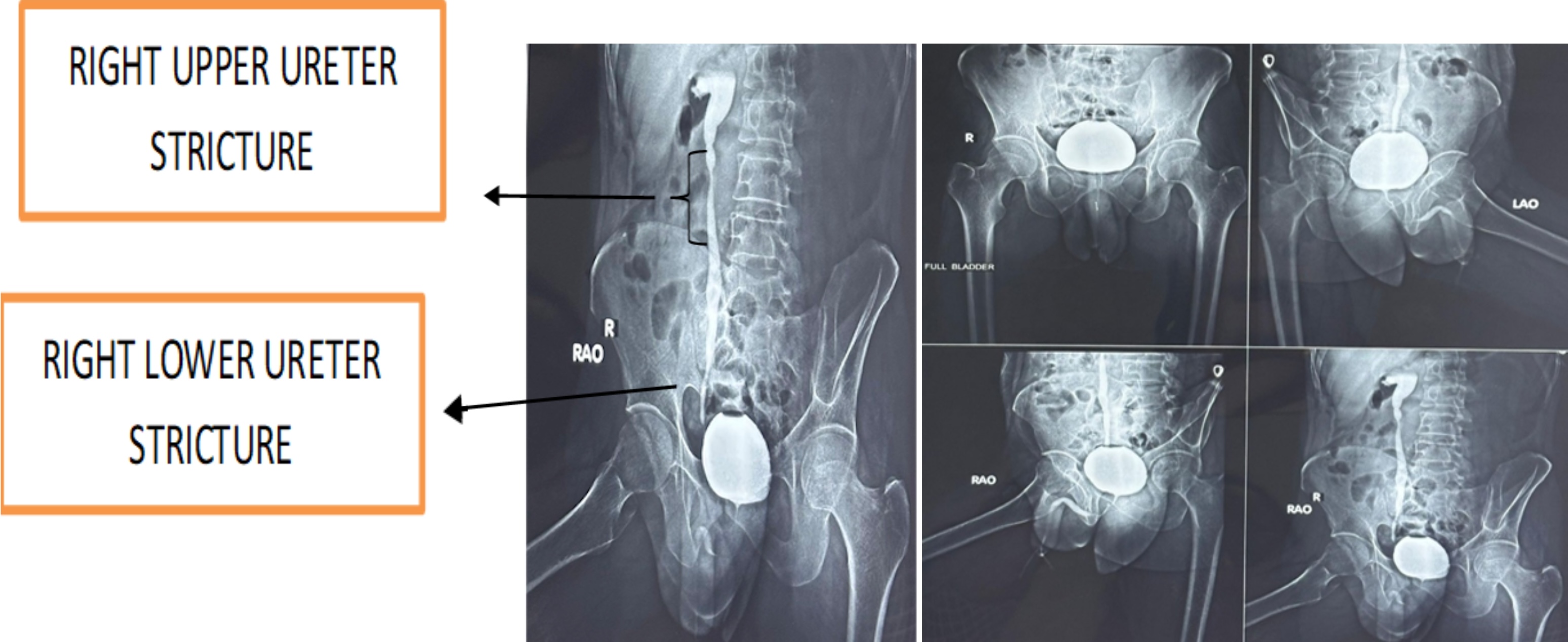
Micturating cystourethrogram: Micturating cystourethrography (MCU) demonstrated a small-capacity, smooth-walled urinary bladder without vesicoureteral reflux. The right ureter appeared irregular and narrowed with proximal dilatation, showing impaired contrast ascent. Findings were suggestive of a distal ureteric stricture in the setting of chronic inflammatory pathology, likely genitourinary tuberculosis (Figure 2).
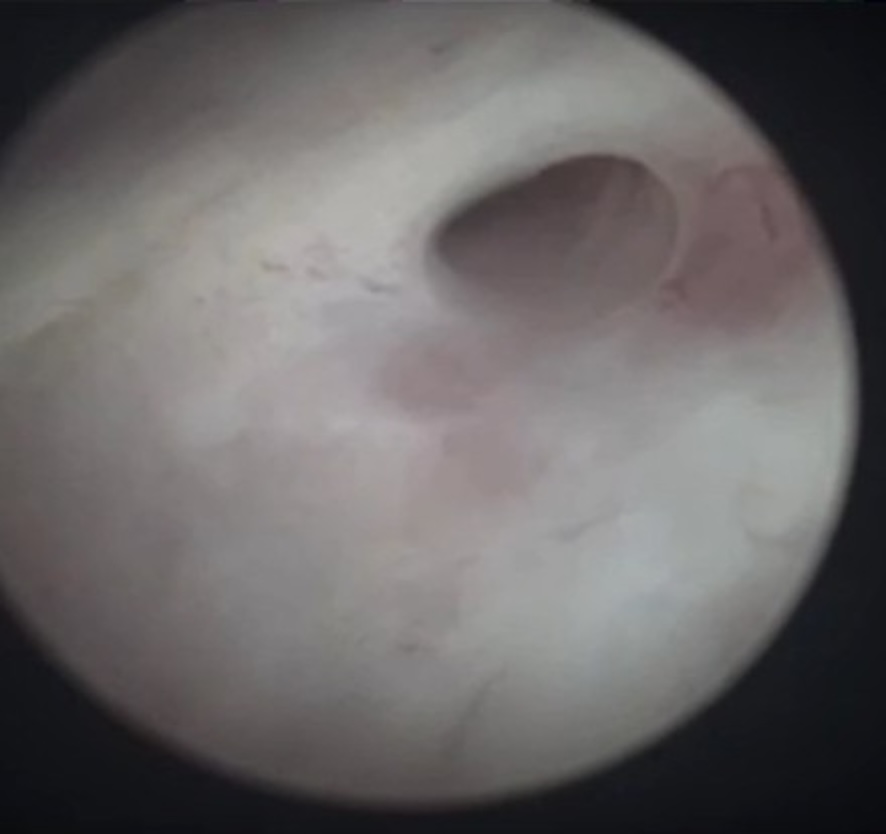
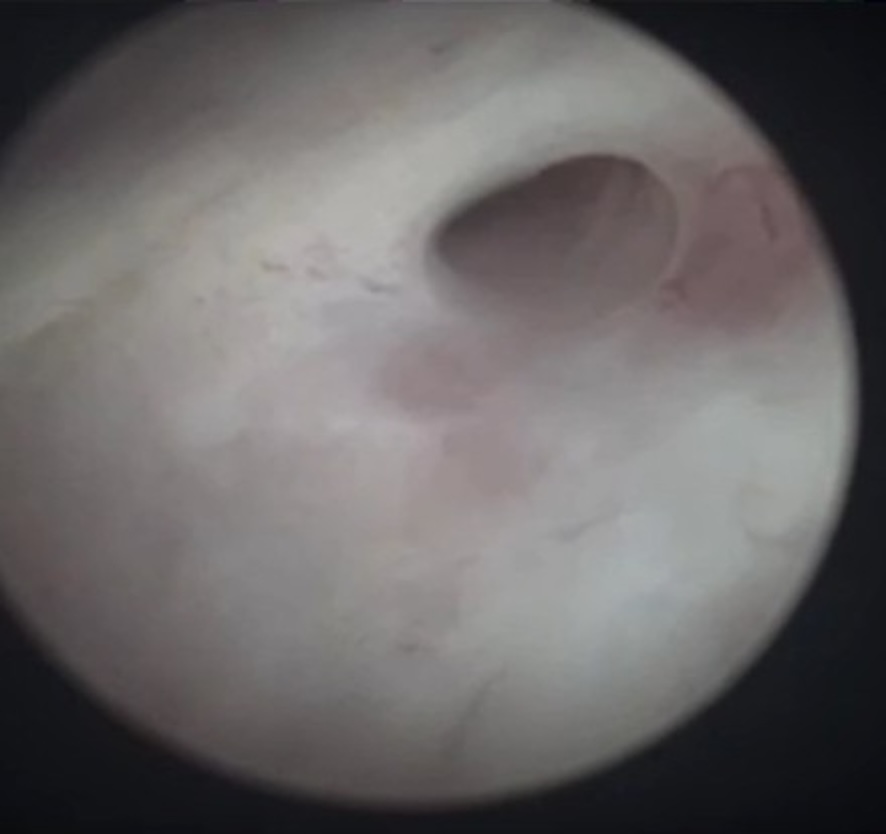
- Cystoscopy: Right lateralized, golf-hole ureteric orifice (Figure 3)
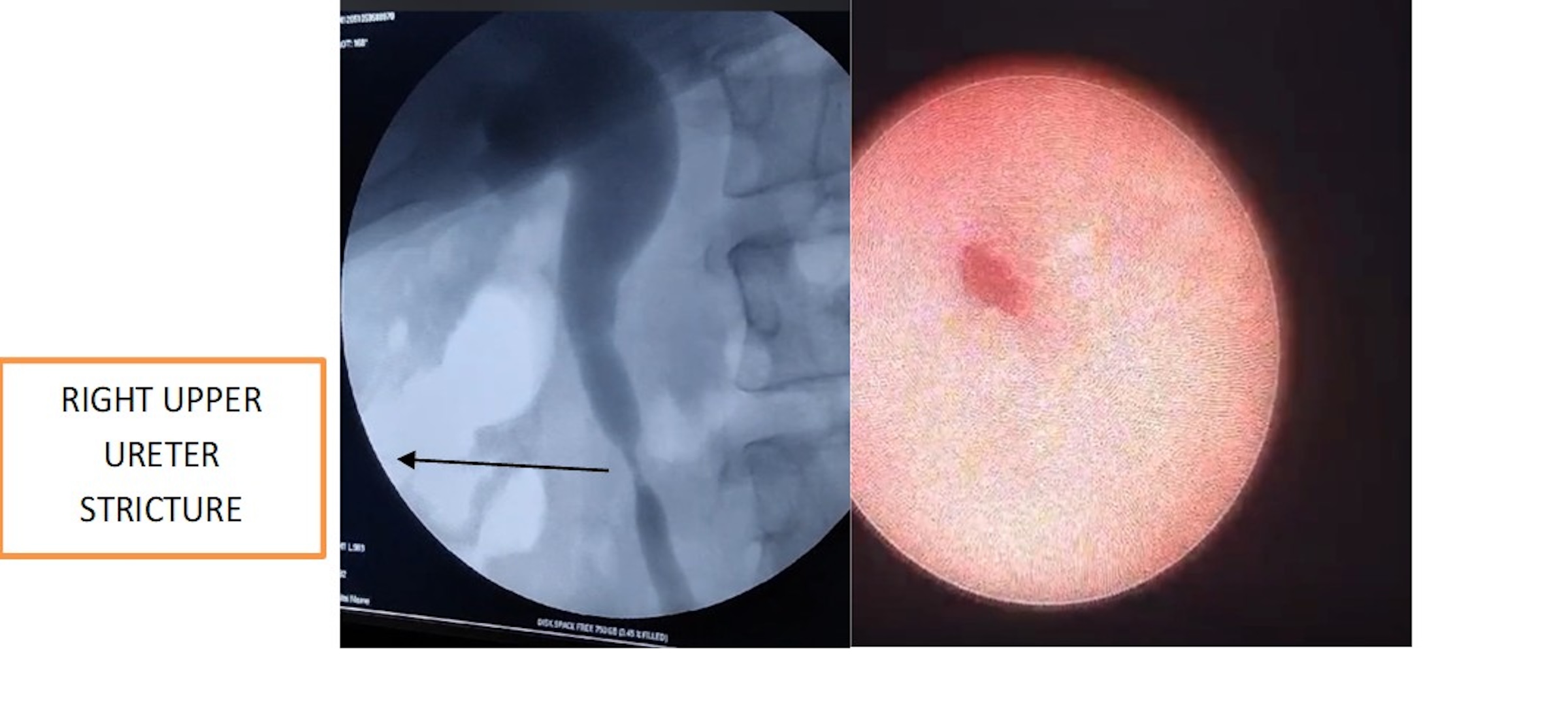
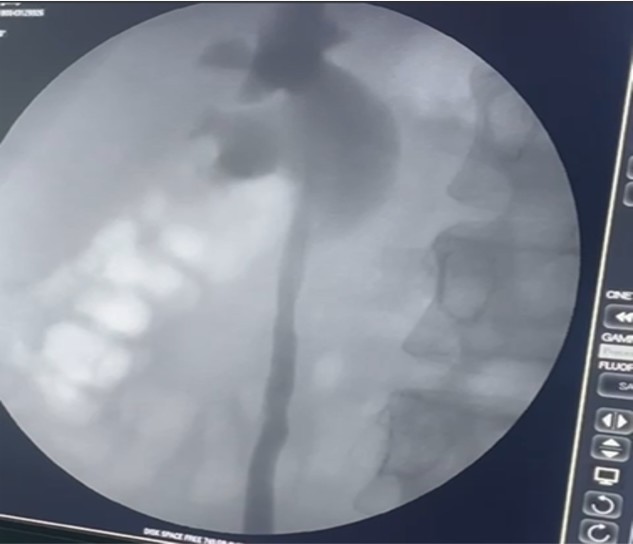
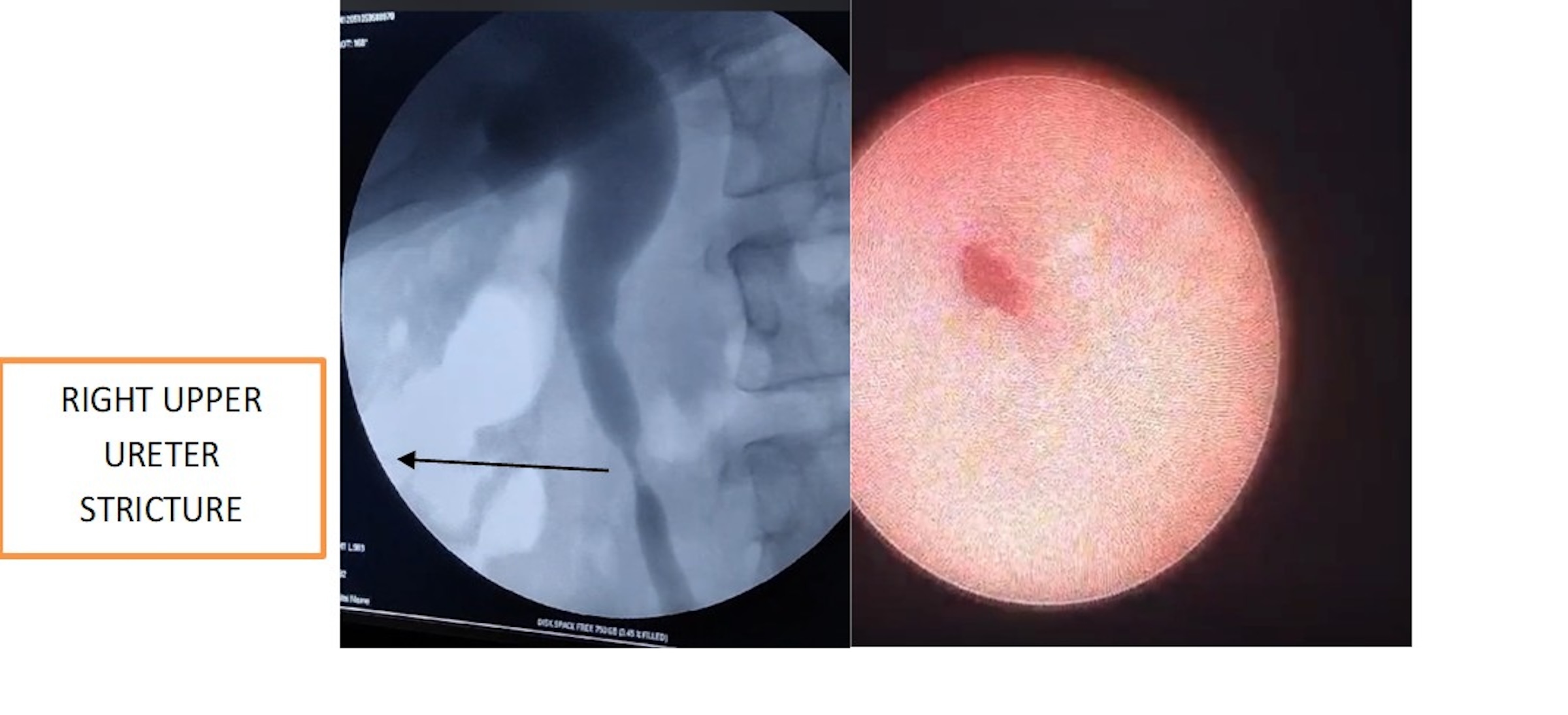
- Retrograde pyelography and ureteroscopy: Preoperative retrograde pyelography revealed irregular segmental narrowing of the right ureter with proximal ureteric and pelvicalyceal dilatation, producing a beaded appearance. There was an associated luminal irregularity with impaired contrast passage across the affected segments. These findings were consistent with a chronic inflammatory stricture, suggestive of genitourinary tuberculosis. (Figure 4)
- Renal scintigraphy: Renal scintigraphy showed a small right kidney with mildly reduced and inhomogeneous cortical function, associated with right-sided hydroureteronephrosis and sluggish yet non-obstructed drainage (split function: 30.4%). The left kidney demonstrates normal size, preserved cortical function, and unobstructed drainage, with an overall GFR of 91 ml/min (split function: 69.6%).
Treatment
Operative Procedure and Follow-up
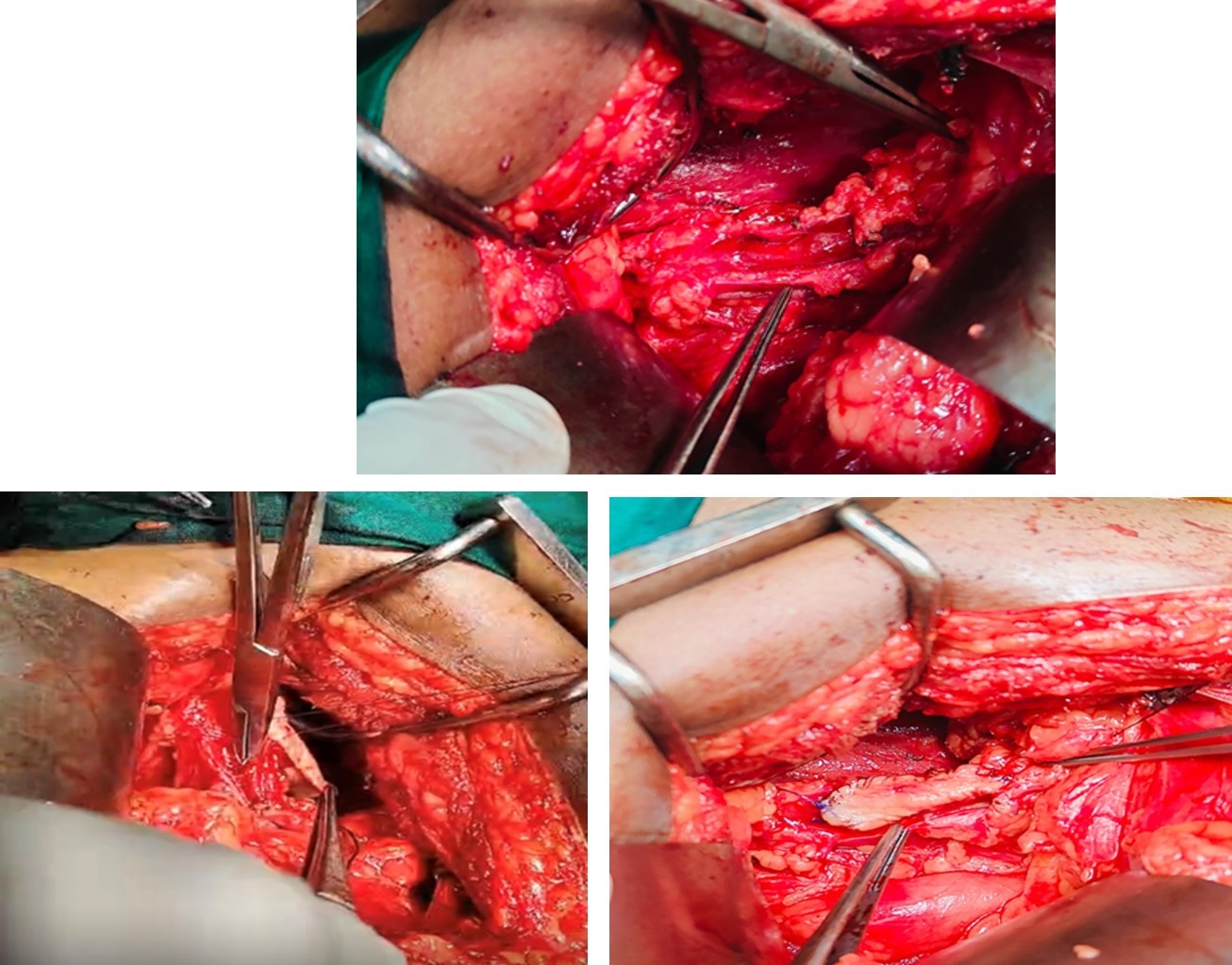
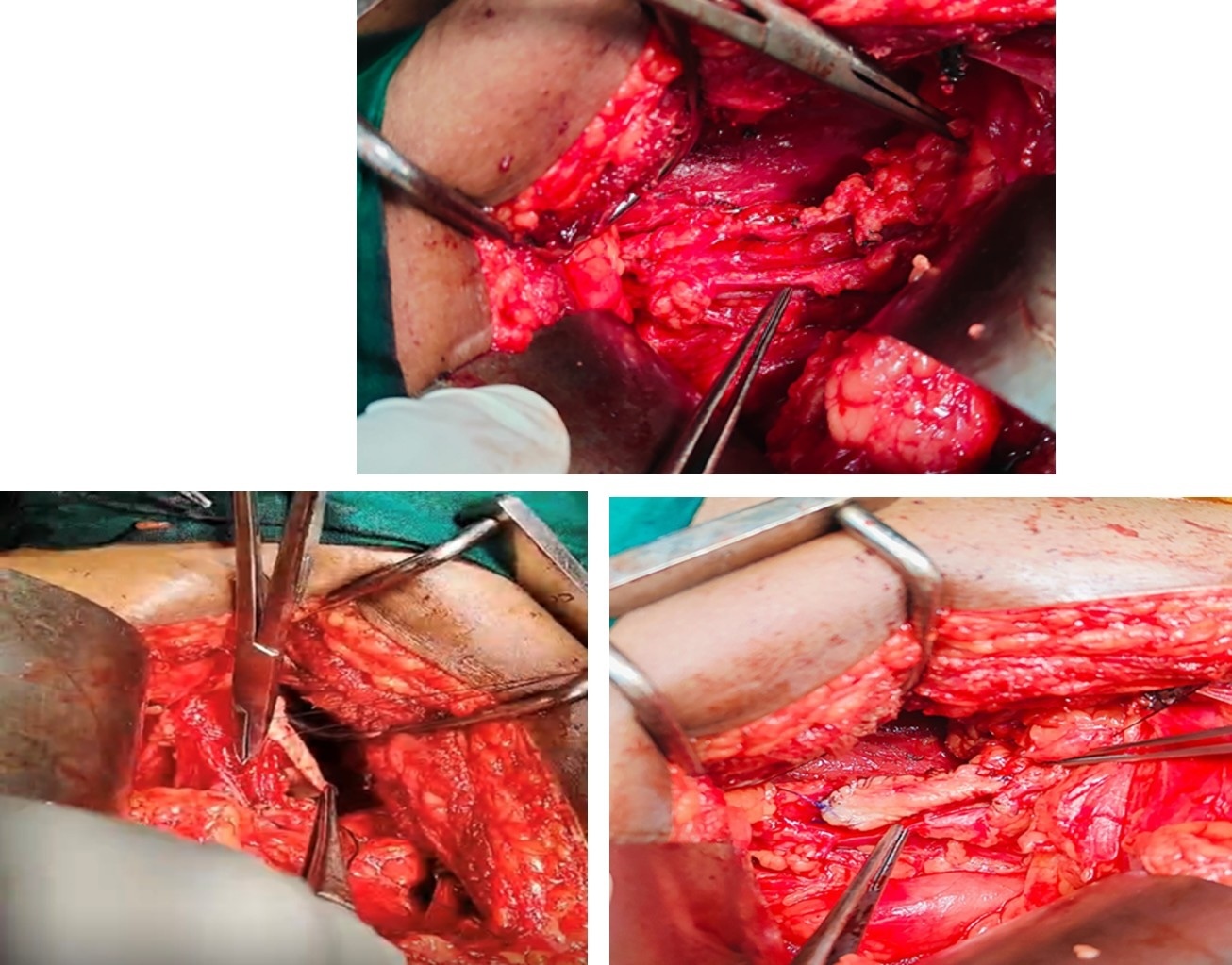
On-table retrograde pyelography (RGP) was performed prior to definitive repair. Under general anesthesia with nasal intubation, a right buccal mucosa graft was harvested after ureteral dissection to determine the required graft length. An elliptical graft (~4 × 2 cm) was obtained from the inner cheek, avoiding the Stensen’s duct and vermilion border, following submucosal infiltration with saline–adrenaline (1:200,000). The graft was harvested in a plane superficial to the buccinator muscle, defatted, and hemostasis secured at the donor site.
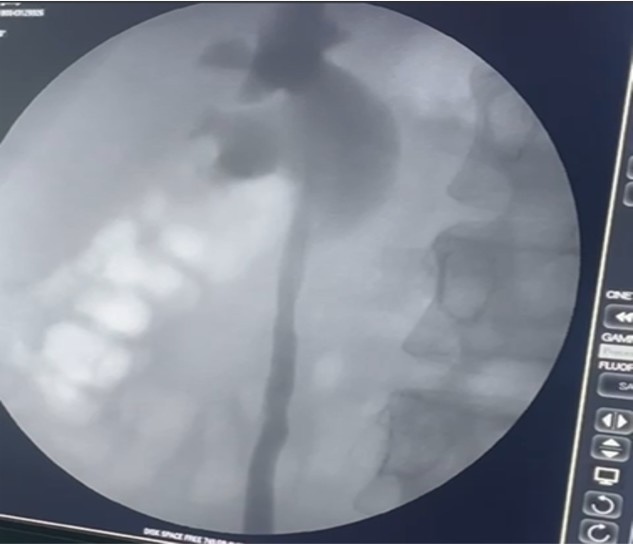
The upper-third ureteric stricture was identified and opened longitudinally (anterior ureterotomy). The buccal mucosa graft was applied as an anterior onlay and sutured with 4-0 polyglactin to achieve mucosa-to-mucosa apposition. A double J stent was placed in an antegrade manner over a guidewire, ensuring appropriate positioning in the renal pelvis and bladder. The graft was supported with periureteric fat quilting. A 20 Fr drain was placed and removed on postoperative day 3; the stent was maintained for 6 weeks. Postoperative imaging confirmed ureteric patency. (Figure 5).
Postoperative Course and Follow-Up
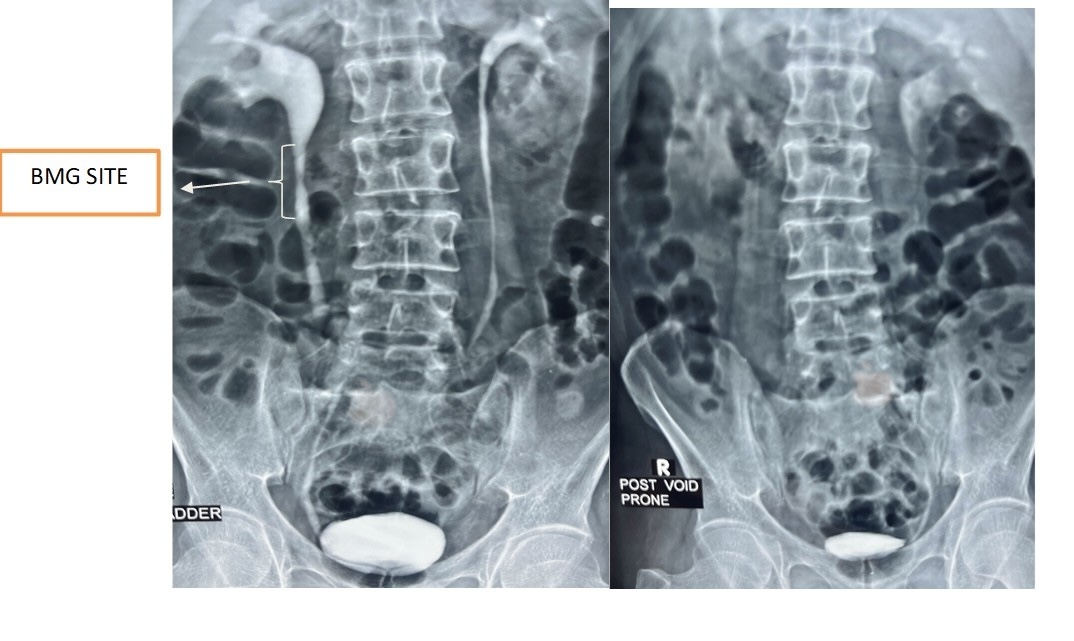
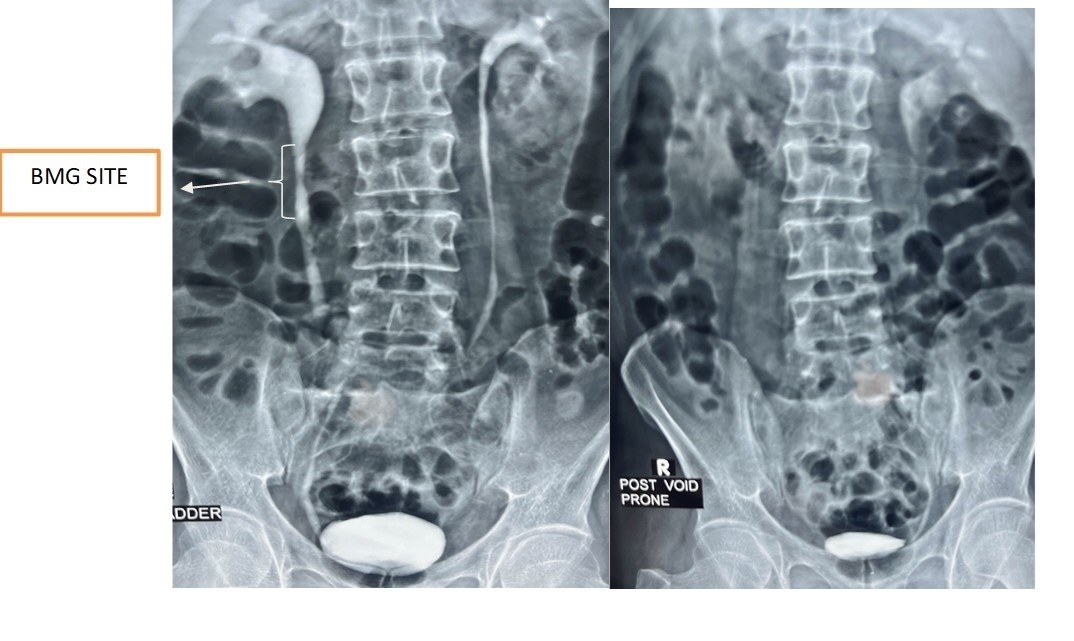
The postoperative period was uneventful. The DJ stent was removed after two months. The patient remained asymptomatic on follow-up, with complete resolution of flank pain and dysuria. Intravenous pyelography performed four months postoperatively showed significant reduction in hydronephrosis with a patent right ureter, indicating successful graft uptake and functional improvement (Figure 7). At 18-month follow-up, the patient demonstrated sustained ureteral patency with favourable clinical and radiological outcomes (Figure 6).
Discussion
Ureteric strictures following genitourinary tuberculosis (GUTB) arise from chronic granulomatous inflammation leading to dense fibrosis and luminal narrowing. While distal ureteric involvement is more frequent, upper ureteric strictures are technically more demanding due to reduced ureteral mobility, periureteric scarring, and impaired vascularity. Surgical decision-making is therefore influenced by stricture length, location, renal function, and local tissue condition.
Buccal mucosa graft (BMG) ureteroplasty has gained increasing acceptance as a reconstructive option, particularly for long-segment or complex strictures where primary anastomosis is not feasible. Reported success rates for BMG ureteroplasty range from approximately 80% to 95%, with durable patency and low complication rates across open, laparoscopic, and robotic approaches.3–5 The favorable outcomes are attributed to the inherent properties of buccal mucosa, including a thick epithelium, rich vascular plexus, and resistance to infection and urine exposure. Recent series have demonstrated comparable efficacy to traditional reconstructive methods, with the added advantage of avoiding bowel-related morbidity and preserving renal units.5–7
Conventional alternatives include ureteroureterostomy for short-segment strictures, which offers high success rates but is limited by tension-free anastomosis requirements. For longer defects, ileal ureter substitution provides a reliable option, although it is associated with metabolic complications, mucus production, and long-term morbidity. The Boari flap, often combined with a psoas hitch, remains useful for mid- to distal ureteric defects but is less suitable for proximal strictures. Renal autotransplantation and nephrectomy are generally reserved for highly complex or non-salvageable cases. In the present case, the lower ureteric segment was amenable to endoscopic negotiation, whereas the upper ureteric stricture necessitated reconstruction. The use of perinephric fat as a vascularized bed for graft reinforcement allowed adequate graft uptake while maintaining an extraperitoneal approach, thereby minimizing intra-abdominal morbidity.3,4
Long-term outcomes in such cases are encouraging, with sustained ureteral patency and preservation of renal function reported in most series. Continued follow-up with imaging and functional assessment remains essential, particularly in the context of underlying tuberculosis and the potential for recurrence or associated vesicoureteral reflux, which should be managed based on clinical progression.
Limitations
As a single-case report, the findings have limited generalizability and cannot establish comparative efficacy or causality. Outcomes may be influenced by patient-specific factors and operator expertise, underscoring the need for larger, controlled studies.
Conclusion
Ureteric strictures remain a significant complication of genitourinary tuberculosis and may lead to progressive renal damage if inadequately treated. Buccal mucosa graft ureteroplasty offers a safe, effective, and durable reconstructive option for complex upper ureteric strictures, avoiding the morbidity associated with bowel interposition or renal autotransplantation. This technique should be considered a valuable addition to the reconstructive armamentarium for post-tubercular ureteric strictures.