Introduction
Hemolymphangioma is an uncommon benign neoplasm, either congenital or acquired in origin, characterized by the dilation of lymphatic vessels accompanied by extravasation of erythrocytes and fibrosis. This tumor predominantly arises within the soft tissues of the neck, axilla, thorax, and lower limbs.1 It primarily affects pediatric populations, particularly neonates and infants, and is frequently associated with congenital anomalies of the vascular and lymphatic systems. Reports of hemolymphangioma involving the rectum are exceedingly rare. Only three cases of rectal hemolymphangioma have been documented in the literature, the most of which have diffuse lesions. Only one occurrence of hemolymphangioma was identified in the lower rectum.1 It is often difficult to distinguish hemolymphangioma from other space-occupying rectal diseases, making preoperative and intraoperative diagnosis extremely complex. No studies have detailed its magnetic resonance imaging (MRI) features. Clinically, rectal hemolymphangioma may manifest with symptoms such as bleeding, tenesmus, rupture, and/or infection.
Case report
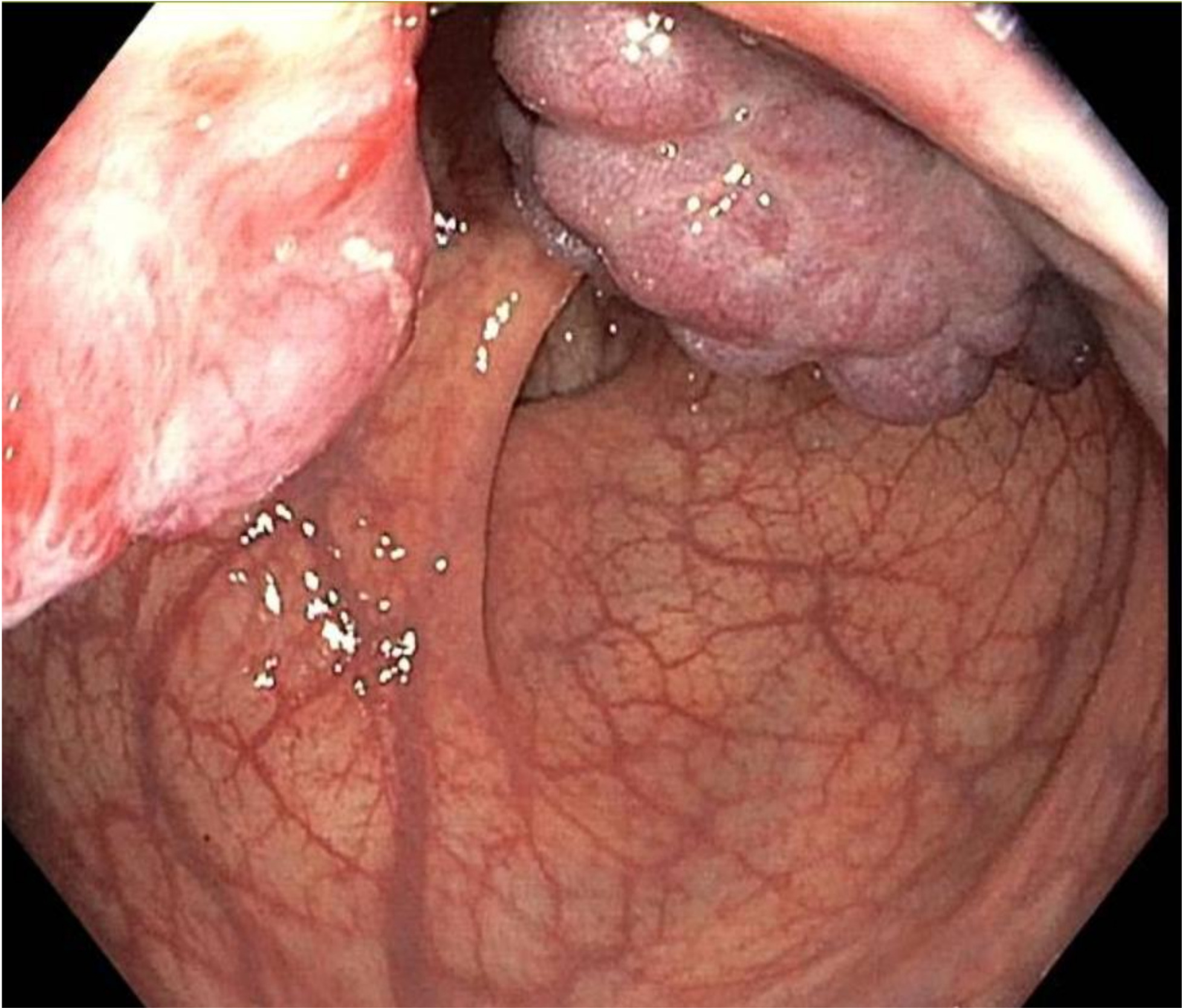
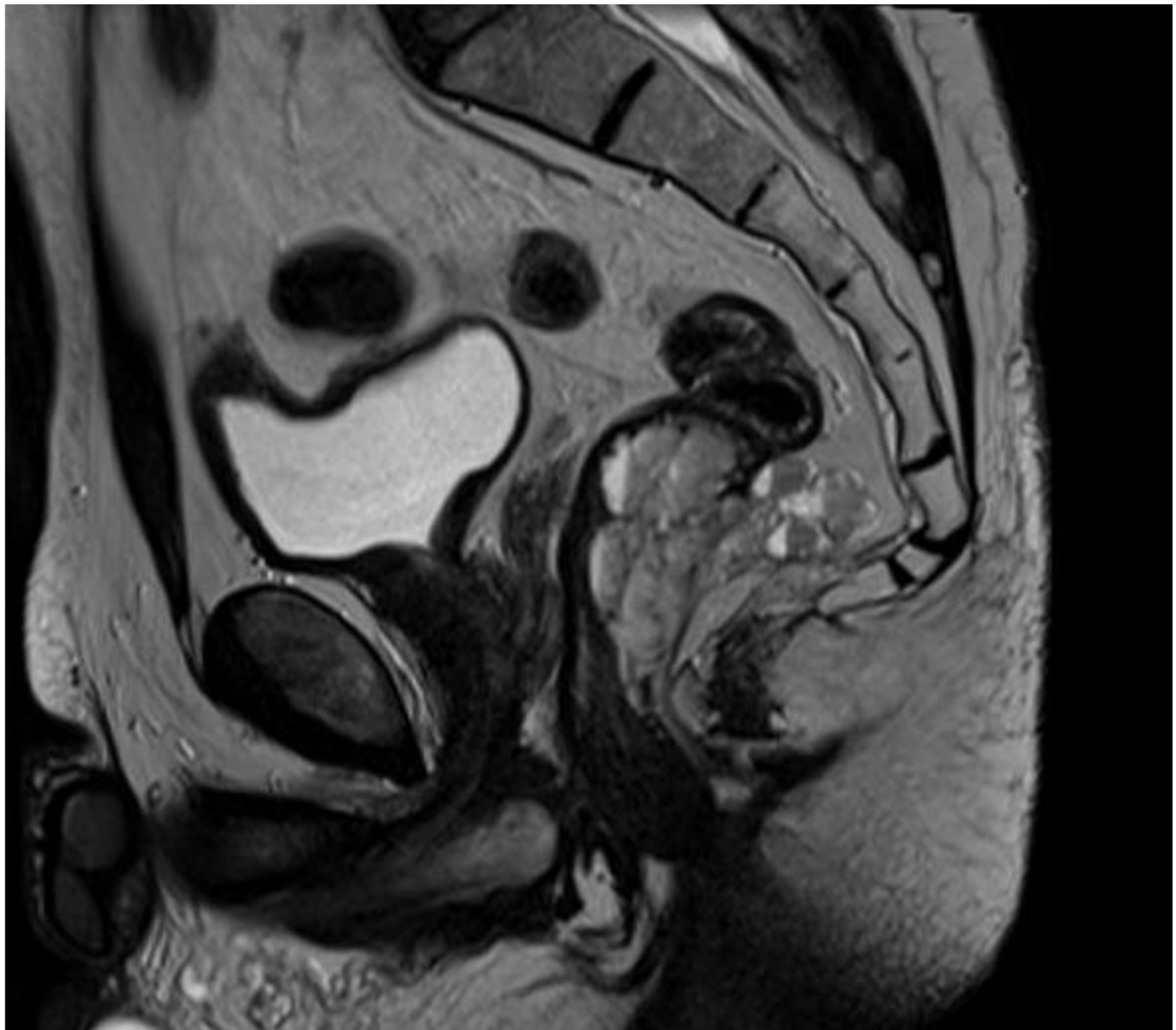
We report the case of a 52-year-old male patient in whom a vegetative lesion of the distal rectum was incidentally identified during urological evaluation for bladder carcinoma. The patient’s medical history was notable for episodes of hematochezia, which had not previously undergone proctological assessment. Endoscopic investigations were conducted (Figure 1); however, biopsy specimens yielded non-diagnostic results. Computed tomography (CT) imaging demonstrated apparent obliteration of the distal rectal lumen by a parietal mass measuring approximately 4 cm. To further characterize the lesion, contrast-enhanced MRI was performed, confirming the presence of an expansive mass in the distal rectum (Figure 2).

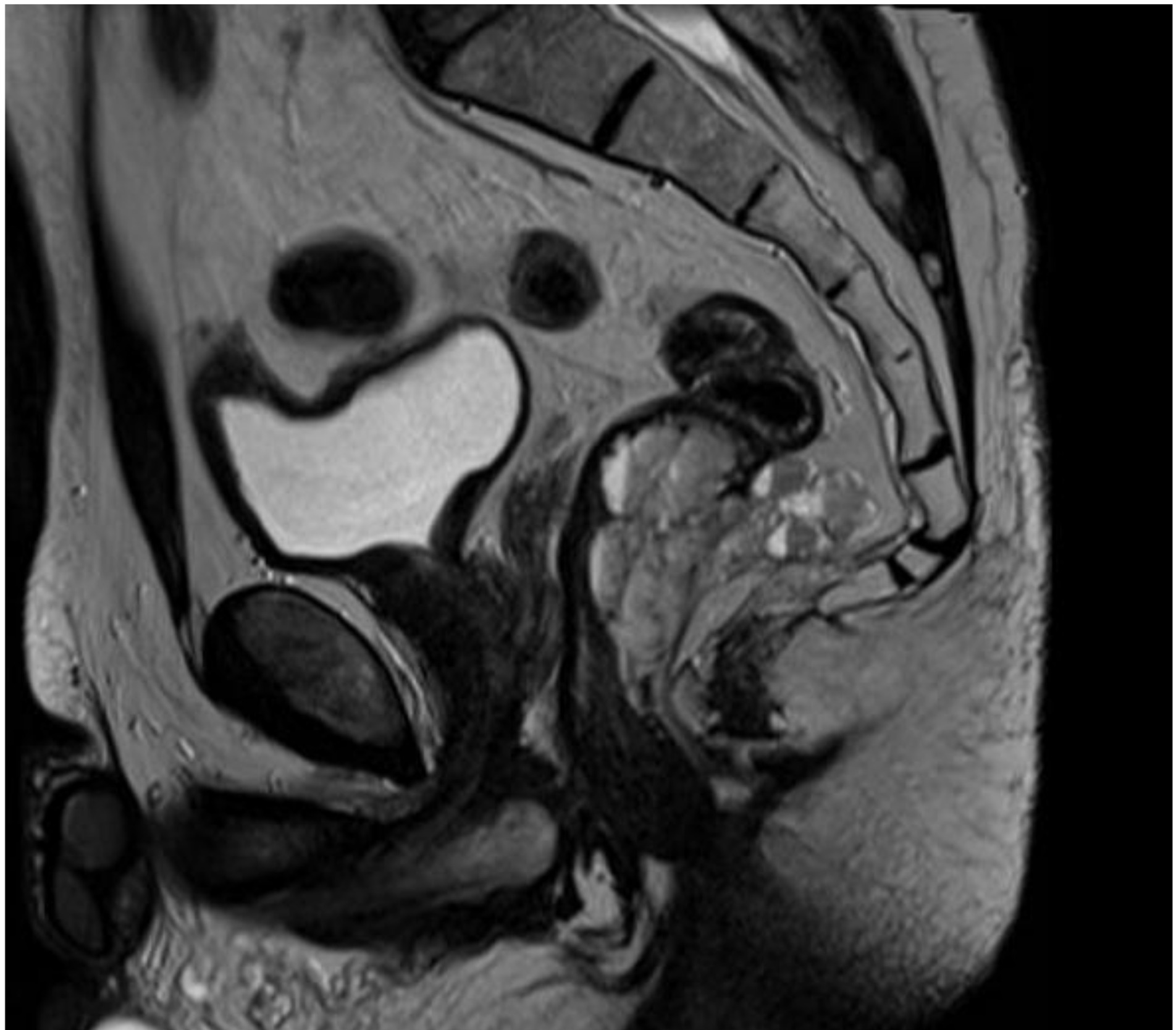
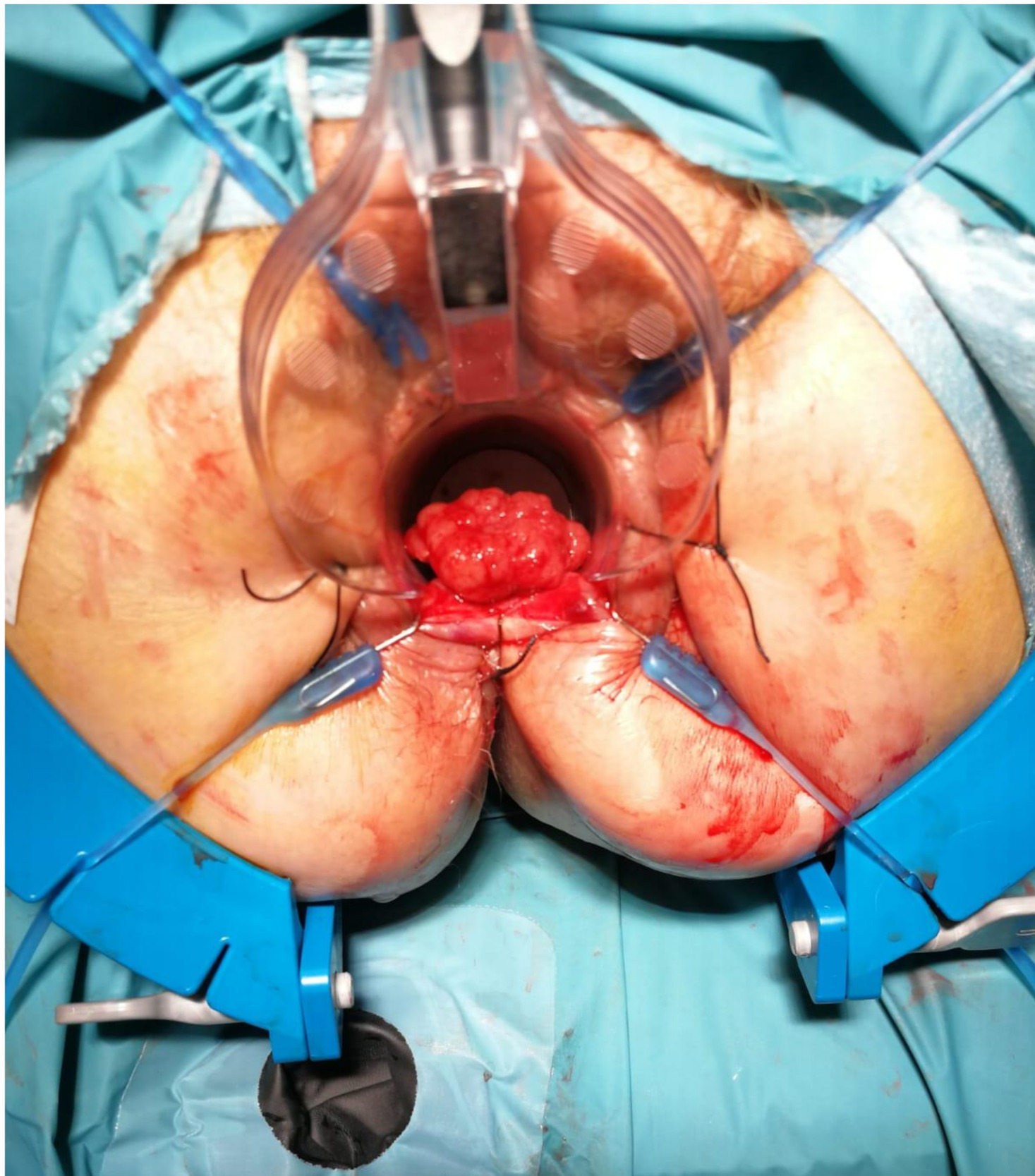
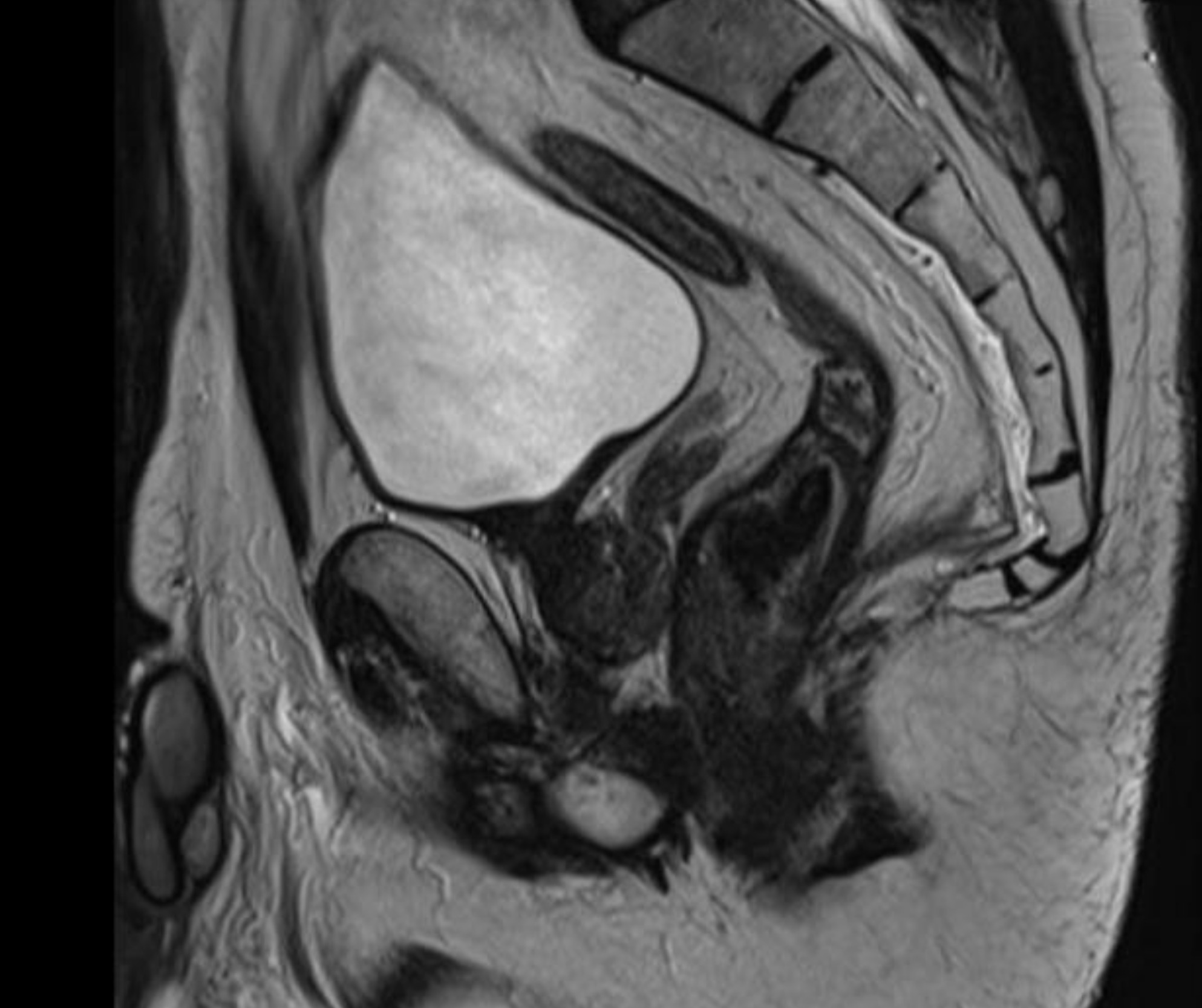
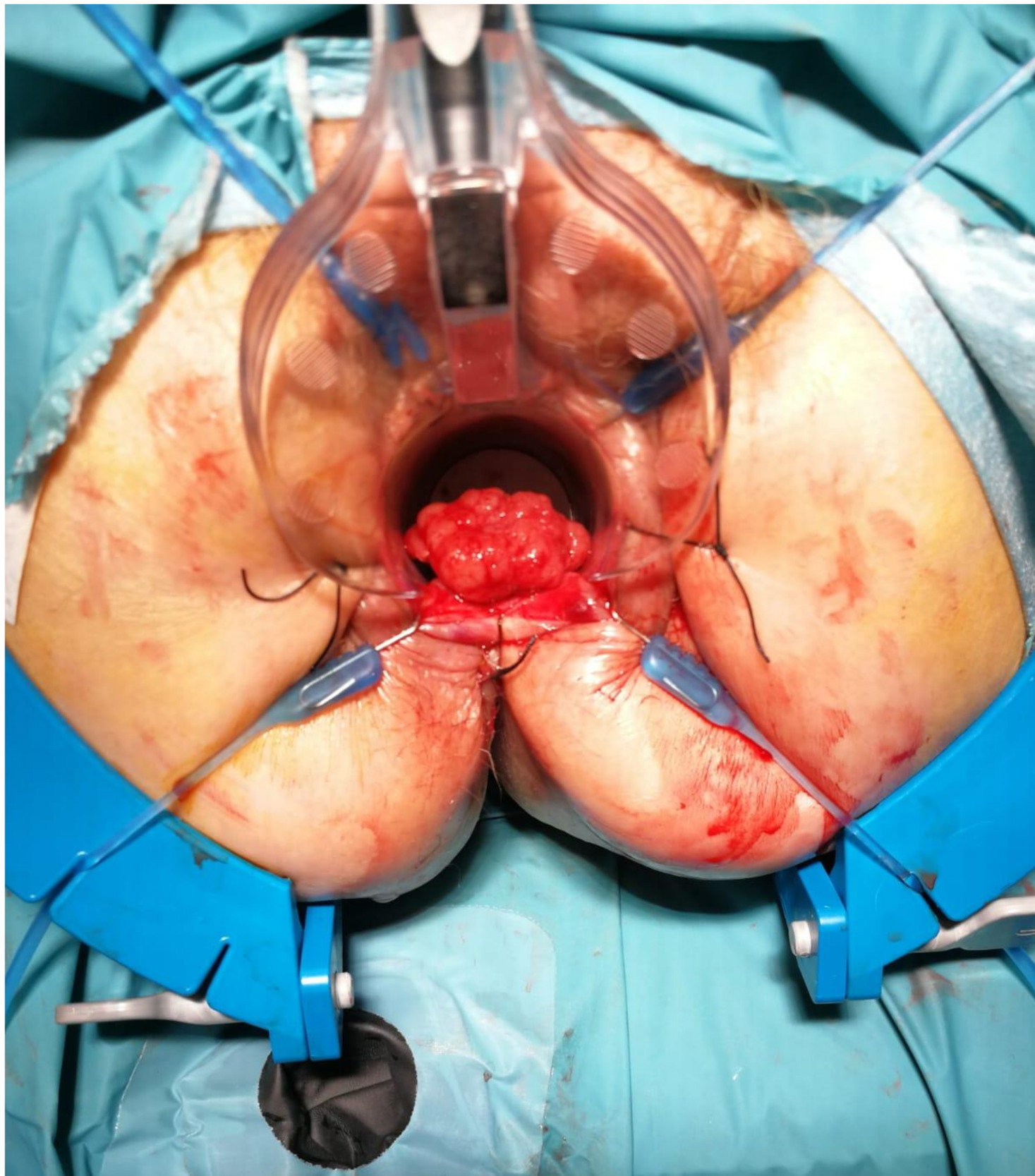
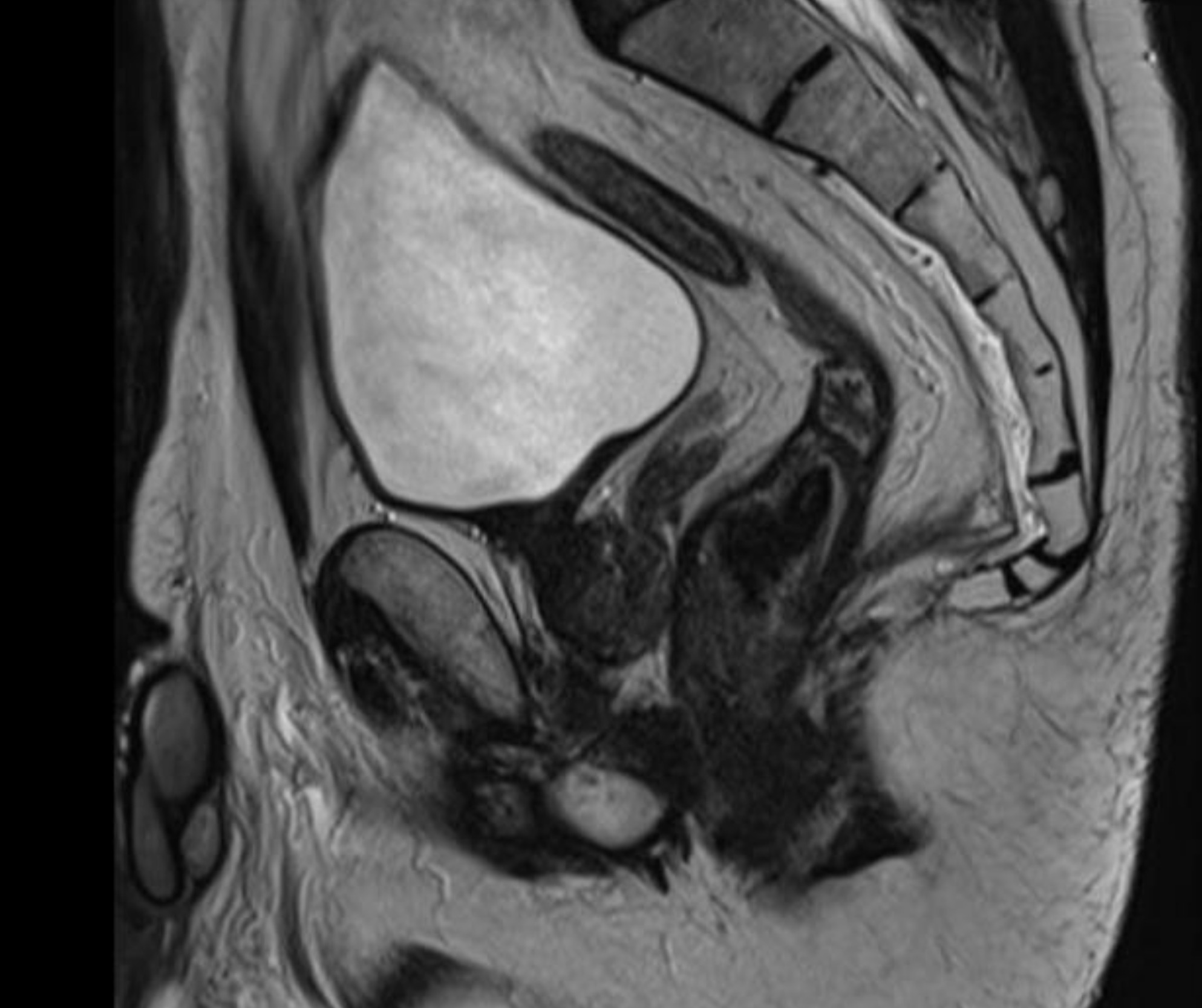
Inhomogeneous signal hyperintensity in T2-weighted sequences with a fluid/fluid level appearance, isointensity signal in T1-weighted sequences, no signal reduction in T1-weighted sequences in opposition of phase in agreement with the absence of a lipid component, no signs of signal restriction in diffusion (ADC 1.6), thin peripheral contrast enhancement, and thin septa in the structure were all features of the MRI. The lesion on the right posterolateral side appeared to affect the muscular coat, extending to the serosa raising suspicion for a teratomatous-type lesion. Following multidisciplinary consultation, surgical excision was planned. A transanal local excision was performed under general anesthesia (Figure 3). The patient’s postoperative course was uneventful, and he was discharged on the first postoperative day. Histopathological analysis revealed an edematous, ulcerated, and chronically inflamed segment of the large intestinal wall, containing lymphatic and intraparietal blood vessel ectasias consistent with hemolymphangioma. No postoperative complications were observed. The patient underwent regular follow-up evaluations, including proctological examinations, CT scans, and MRI studies (Figure 4) every six months for the initial two years, followed by annual assessments. At four years postoperatively, there is no evidence of disease recurrence.
Discussion
Hemolymphangioma represents a rare clinical entity, predominantly congenital in nature, with an incompletely understood pathogenesis.1 Its differentiation from other rectal space-occupying lesions is often challenging, complicating both preoperative and intraoperative diagnostic processes. Preoperative diagnosis primarily depends on colonoscopic evaluation and imaging modalities. Complete surgical excision remains the treatment of choice and is considered the most effective therapeutic strategy.2 Although minimally invasive transanal approaches have not been previously documented in the literature for this condition, the preservation of sphincter function during surgical management is of paramount importance. Haemolymphangioma of the rectum represents a rare vascular and lymphatic malformation, typically manifesting as recurrent, painless rectal hemorrhage. Preoperative imaging studies are essential for establishing an accurate diagnosis and guiding the surgical management plan. While the recurrence rate after partial resection ranges from 50% to 100%, the recurrence rate after fully resection is low, ranging between 10% and 27%. In addition as a consequence, routine postoperative monitoring is necessary. There have been documented experiences of patients being treated surgically utilizing extremely damaging procedures, commonly for the reason of an uncertain diagnosis or a suspicion of malignancy. Local-regional excision is the best approach for this type of lesion, as we believe the goal of treatment should be achieving an adequate functional outcome. Following comprehensive tumor assessment, a minimally invasive surgical approach is advised. Transanal excision constitutes an effective technique for the treatment of such lesions, functioning simultaneously as a diagnostic and therapeutic intervention.
Ethical statement
Our institution does not require ethics approval for reporting individual cases or case series
Written informed consent was obtained for anonymized patient information to be published in this article.