1. Introduction
Myoglobin cast nephropathy (MCN) causing Acute kidney injury (AKI) is one of the most serious life-threatening complication of both traumatic and non-traumatic rhabdomyolysis. Generally, it occurs in 7 to 10% cases of severe rhabdomyolysis.1 In one study done on 475 cases with rhabdomyolysis, the AKI was seen in 46 cases. Mortality rate among these patients varied between 3.4-59% depending upon presence or absence of renal failure and 80% cases had long- term survival.2
Aetiology of rhabdomyolysis differs among western and tropical countries. In the western countries, Illicit drugs and alcohol are the commonest causes while in the Indian scenario, it commonly occurs due to unaccustomed strenuous physical exertion, snake envenomation, seizures, wasp sting and infections.1–3 Despite its potentially severe consequences, MCN is frequently underrecognized in clinical practice due to nonspecific symptoms and overlapping features with other causes of AKI.
2. Materials and Methods
In our retrospective observational study, we analysed the varied presentations, clinicopathological characteristics, diagnostic approaches, and treatment strategies of all suspected cases of rhabdomyolysis at a tertiary care hospital in western india.
Medical records of renal biopsy samples from Jul 2022 to Jun 2025 were reviewed including samples taken during post mortem examination of cases died due to suspected rhabdomyolysis. Rhabdomyolysis was clinically suspected when patients presented with either oliguria, red brown urine or muscle cramps along with clinical history and laboratory findings. All clinical data at the time of performing the renal biopsy were recorded in a predesigned proforma. Case selection was strictly as as per inclusions and exclusion criteria of the study
2.1. Inclusion criteria
-
Patients diagnosed with acute kidney injury (AKI) during the study period (July 2022–June 2025), as defined by KDIGO criteria (increase in serum creatinine and/or reduced urine output).
-
Renal biopsy specimens showing pigment casts on light microscopy, suspicious for myoglobin cast nephropathy.
-
Immunohistochemical confirmation of myoglobin positivity within tubular casts on renal biopsy.
-
Clinical or biochemical evidence of rhabdomyolysis, including markedly elevated serum creatine phosphokinase (CPK) levels.
-
Patients of all age groups and both sexes (if applicable), treated at the study institution during the specified study period.
-
Availability of complete clinical, biochemical, histopathological, and follow-up data in hospital records.
2.2. Exclusion criteria
-
Renal biopsies showing pigment casts negative for myoglobin on immunohistochemistry (e.g., hemoglobin casts, bile casts).
-
Cases of AKI due to other confirmed etiologies without histological evidence of myoglobin cast nephropathy (e.g., acute tubular necrosis without pigment casts, glomerulonephritis, thrombotic microangiopathy).
-
Inadequate or insufficient renal biopsy tissue for histopathological evaluation or immunohistochemical staining.
-
Patients with pre-existing chronic kidney disease (CKD) with documented baseline renal dysfunction prior to the episode of rhabdomyolysis, unless superimposed acute pathology could be clearly distinguished.
-
Incomplete medical records lacking essential clinical, laboratory, or outcome data.
-
Duplicate records or repeat biopsies from the same patient during the study period (only the first diagnostic biopsy included).
For light microscopy, formalin fixed paraffin embedded 3–5-micron sections were taken and stained with Haematoxylin and eosin(H&E), Periodic acid – Schiff (PAS) and Masson’s trichrome (MT) stain. Pigment casts were observed in 35 cases. Myoglobin Immunohistochemistry (IHC) using rabbit monoclonal anti-myoglobin antibody, Clone EP87 (PathnSitu, Pleasanton, CA) was performed in these cases for evidence of myoglobin casts. Out of 35 cases, 25 cases (71.42%) showed casts staining positive with IHC for myoglobin. Only those cases with positive myoglobin IHC were included for further study. Cases with suspected clinical diagnosis of rhabdomyolysis but without IHC proven myoglobin casts were not included in this study.
For the study purpose, AKI was classified into three stages, depending on severity, using the KDIGO (kidney disease: improving global outcomes) criteria which included serum creatinine levels and urine output. The KDIGIO is a standardized international classification system which combines two previous classification systems, RIFLE (risk, injury, failure, loss of kidney function and end-stage kidney disease) and AKIN (acute kidney injury network)
2.3. Study Outcome Definitions
Renal Recovery
Acute kidney injury (AKI) was defined and staged (1-3) according to the KDIGO criteria, based on changes in serum creatinine and urine output.
Renal recovery was assessed relative to baseline kidney function and categorized as follows:
-
Complete recovery: Return of serum creatinine to within 0.3 mg/dL of baseline (or to the estimated baseline value when pre-morbid creatinine was unavailable), with independence from renal replacement therapy (RRT), if previously initiated.
-
Partial recovery: Improvement in serum creatinine from peak AKI stage with a reduction of at least one KDIGO stage, but without return to baseline kidney function, and independence from RRT.
-
No recovery: Persistence of AKI without improvement in KDIGO stage or continued dependence on RRT at the time of discharge or last follow-up.
2.4. Statistical Analysis
In Statical Analysis, Continuous variables were expressed as mean ± standard deviation (SD) or mean with interquartile range (IQR) depending on data distribution. Categorical variables were presented as frequencies and percentages.
3. Results
Table. 1 Demographic, clinical, biochemical data, treatment done and outcome
Abbreviations: mg/dL (milligrams per decilitre), IU/L (international units per litre), CPK (Creatinine phosphokinase), LDH (Lactate dehydrogenase)
The aetiologies were varied and nonspecific in all cases. The most common cause was unaccustomed physical exertion seen in 18(72%) cases. (Table 2)
Among all the cases the youngest was of 27 yrs and the eldest case was of 45 yrs. There cases were male and no other co-morbid conditions were seen. All cases presented with AKI and rhabdomyolysis as the possible cause was clinically suspected in 21 out of 25 (84%) cases based on clinical presentation of oliguria, muscle cramps, and cola coloured urine.
All cases showed elevated Serum Creatinine phosphokinase (CPK) with mean value of 2183 IU/ L (normal upper limit of 170 U/L in males and 135 U/L in females). Highest values of CPK were seen in exertional causes like heat stroke cases (> 5500 IU/ L) and smallest with infection related (> 950 IU/ L) causes.
The serum creatinine was elevated in all cases (mean value 7.53 mg/ dl, normal value 0.7- 1.3 mg/ dl) with highest values seen in snake bite case (10.8 mg/ dL). All cases showed hyperuricemia, hyperphosphatemia while serum calcium levels varying between hypo and hypercalcaemia (normal value 8.5- 10 mg/ dl) depending upon timing of the samples.
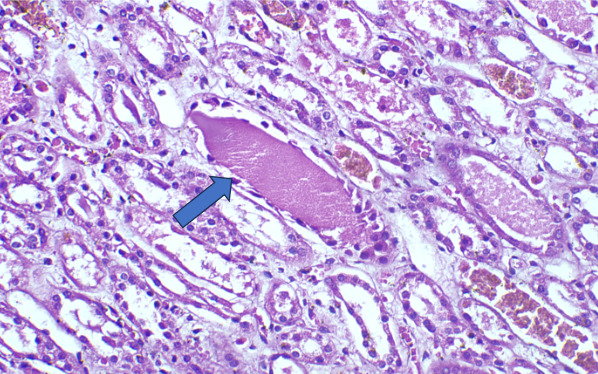
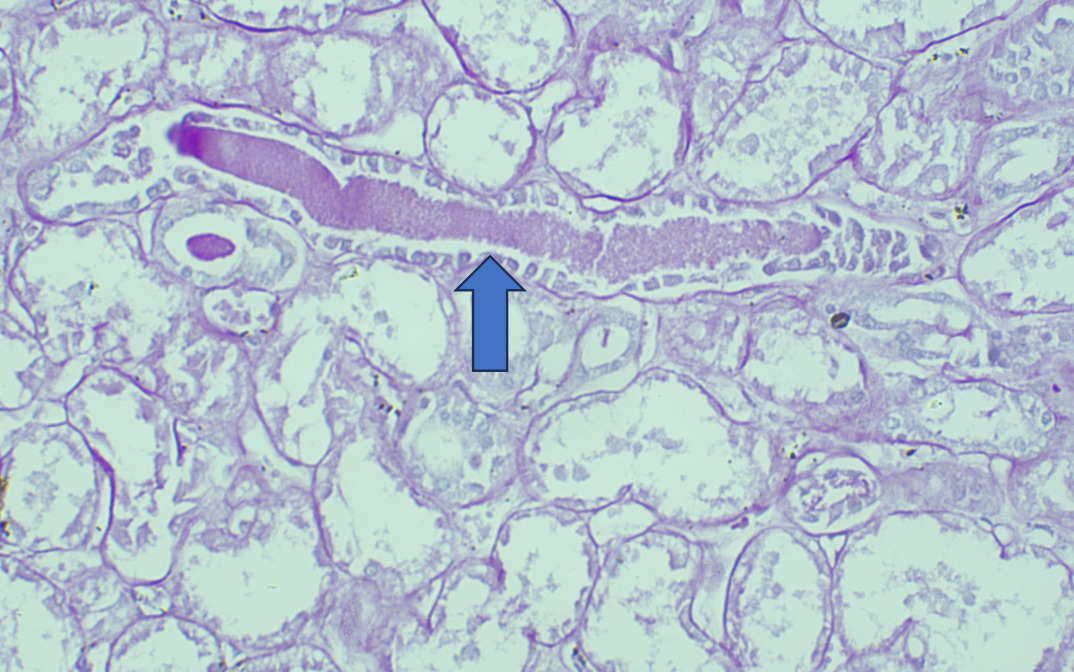
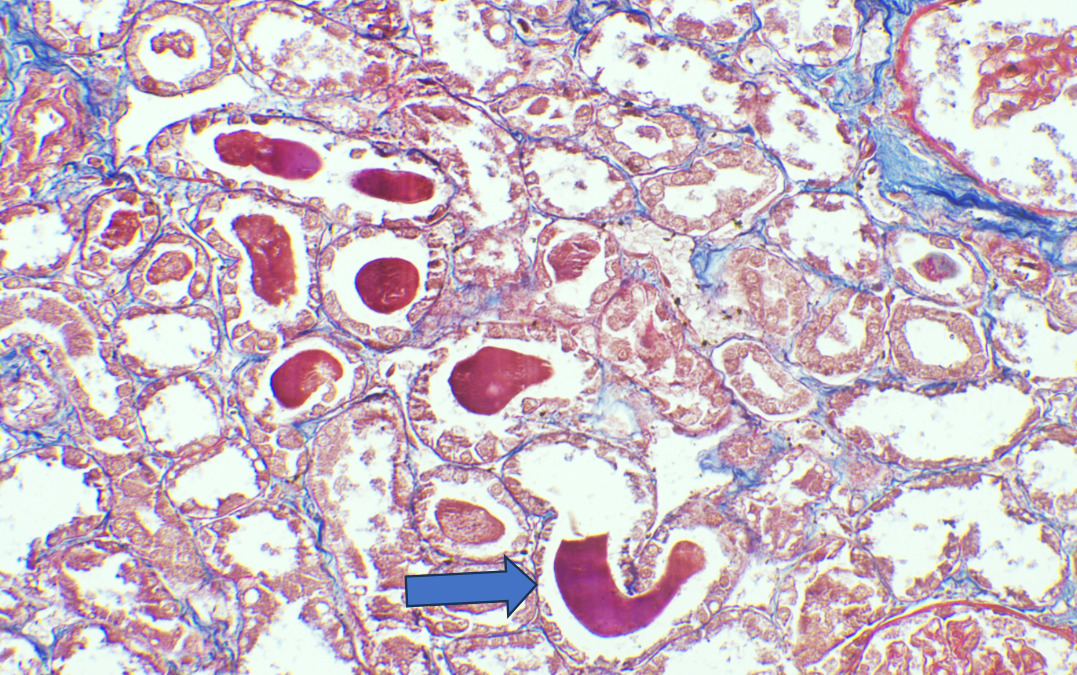
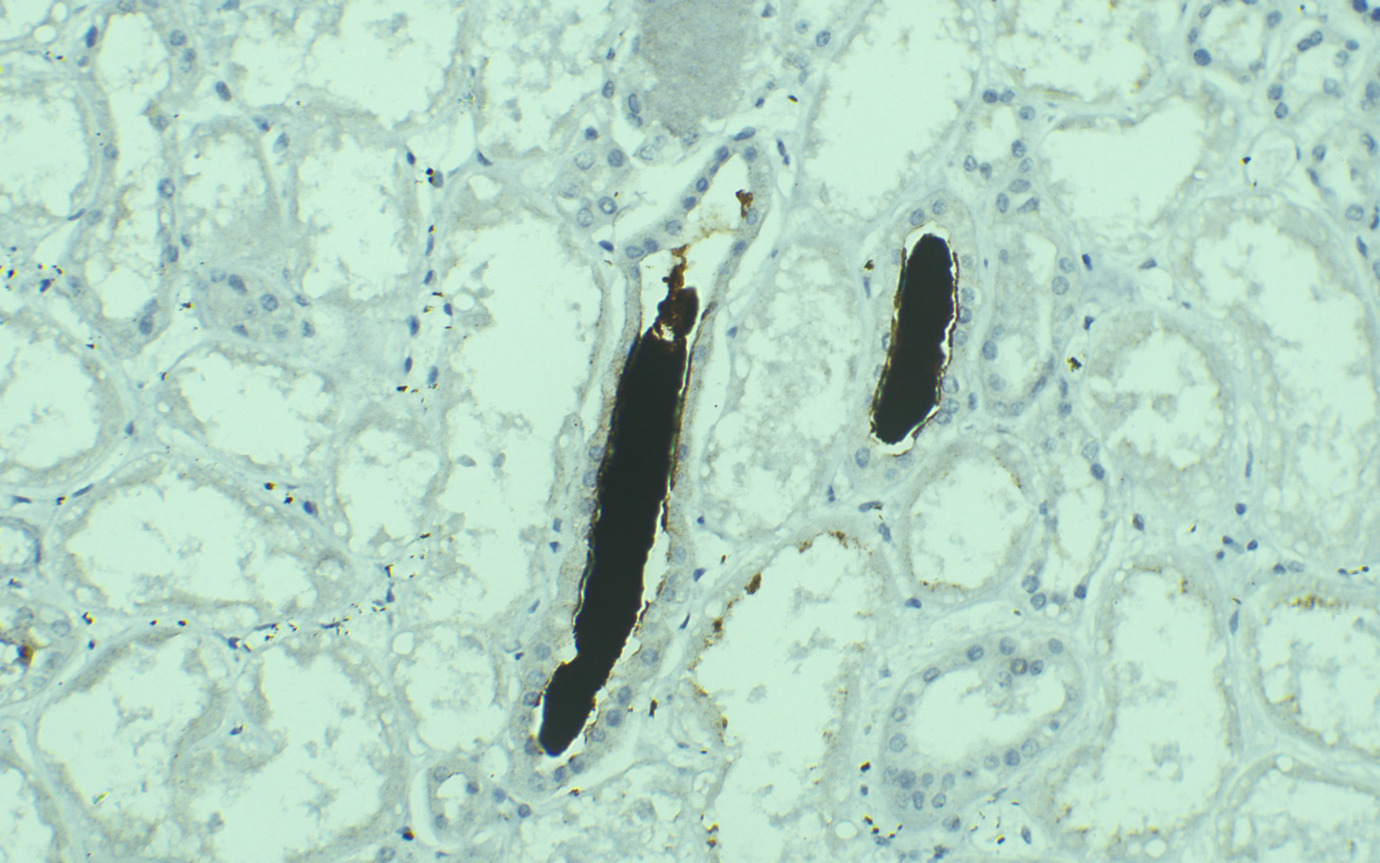
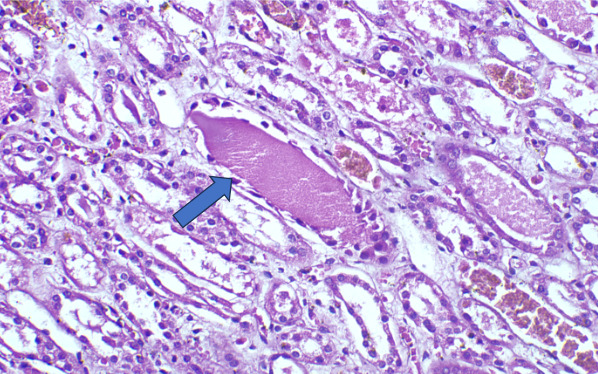
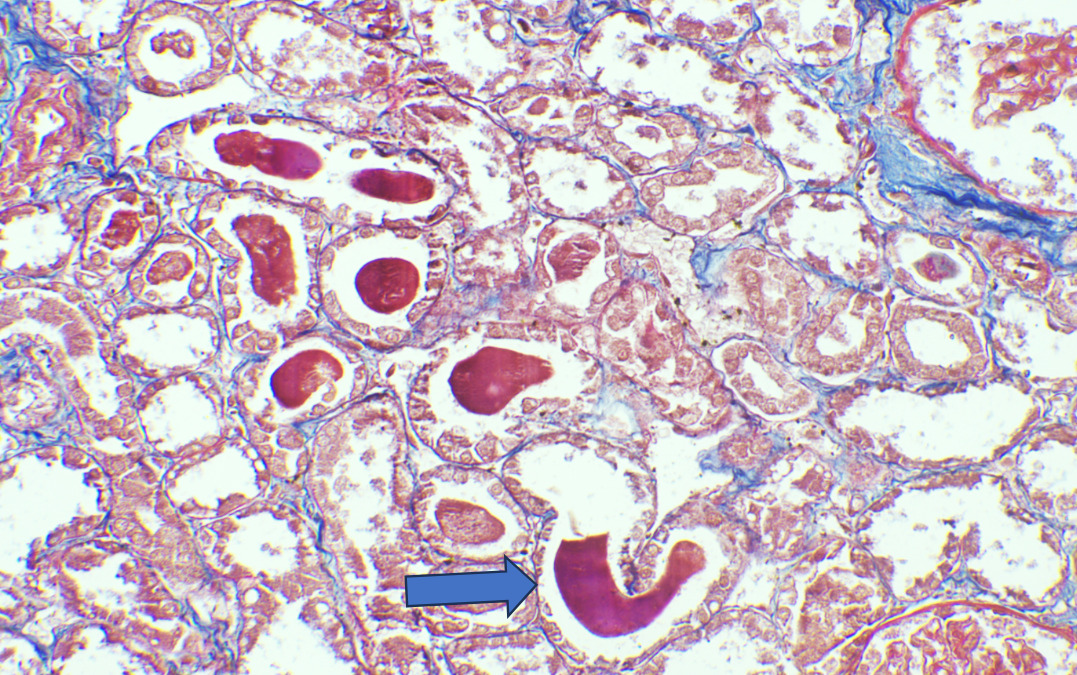
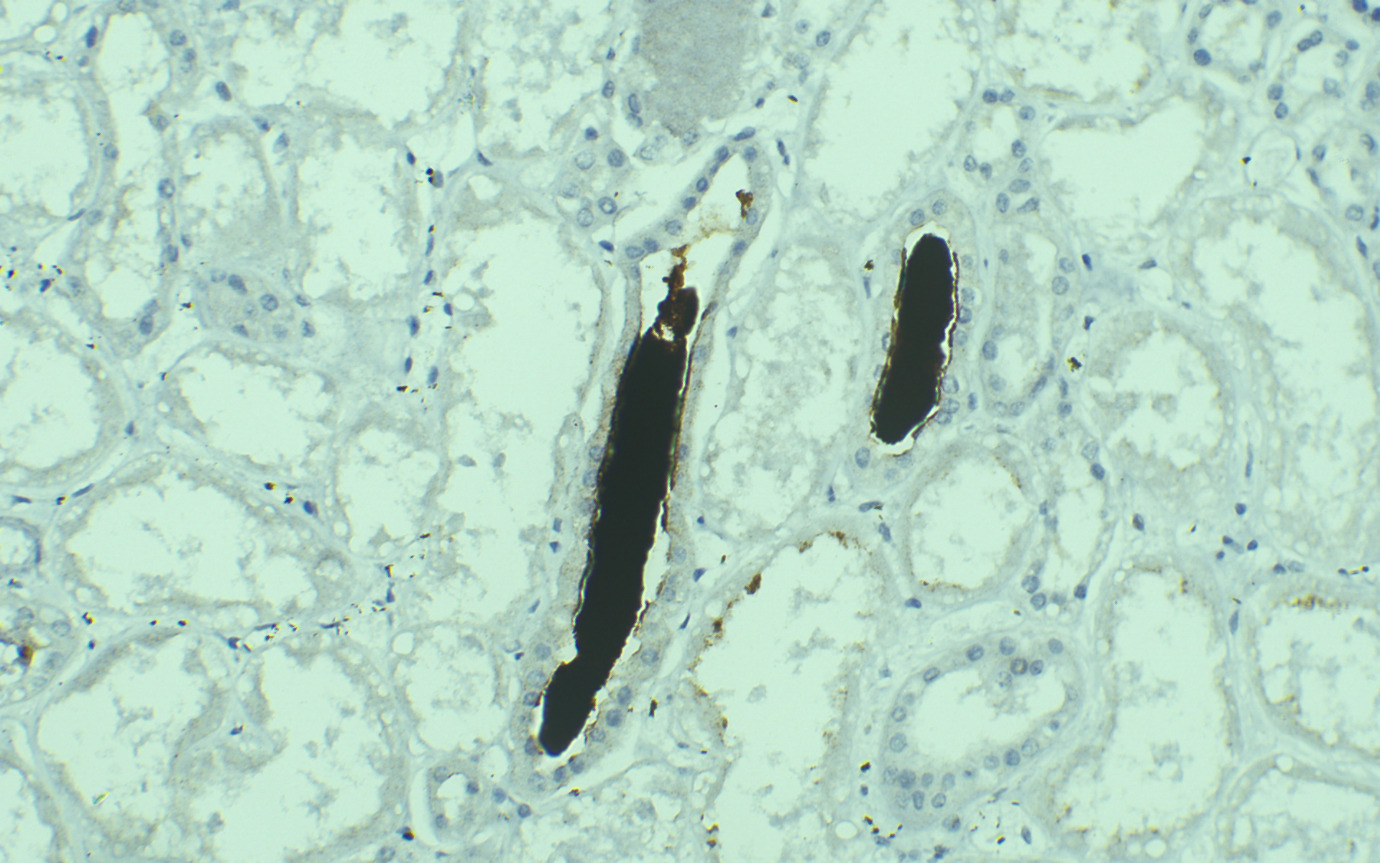
On Light microscopy, The H &E-stained sections of renal biopsy showed features of acute tubular epithelial cell injury with swollen, attenuated lining epithelium. Numerous tubules showed pink to red brown casts in the lumen which were grainy to globular and ropy at places. (Figure 1). The casts appeared weakly PAS positive (Figure 2) and fuchsinophilic on MT stain (Figure 3). On IHC, these casts gave positive staining for myoglobin (Figure 4).
.png)
None of the renal biopsy revealed significant glomerulosclerosis or interstitial fibrosis. Information on the treatment handed and Follow-up details were available for 25 cases.
Twenty-one of them required haemodialysis with an average of 8 sessions per case and four of them were treated with fluid and renal replacement therapy. Twenty- two cases recovered with significant improvement in renal function while 3 cases succumbed to their illness.
4. Discussion
Rhabdomyolysis is characterized by necrosis of striated muscle cells and the release of myoglobin into extracellular space and circulation leading to myoglobinuria in both traumatic or non-traumatic causes.1–4 AKI is a fatal but potentially preventable complication of severe rhabdomyolysis, regardless of the aetiology.
The pathophysiology of rhabdomyolysis encompasses direct sarcolemmic injury, unregulated increase in intracellular calcium and the activation of calcium dependent neutral proteases and phospholipases. Eventually, this leads to lysosomal digestion of myocyte contents and destruction of myofibrillar proteins, resulting in disintegration of the myocyte and release of myoglobin in circulation.4,5
Myoglobin is dark red 17,800 Da oxygen carrier heme (Fe+2) protein which appears in urine above renal threshold of 0.5 -1.5 mg/dl. When a large amount of myoglobin enters the tubular lumen, it precipitates with Uromodulin (Tamm-Horsfall) protein to form myoglobin casts. Acidic urine and volume depletion exacerbates this process. Also, reactive oxygen species released during damage to muscle cells oxidises the ferrous iron (Fe+2) to ferric oxide (Fe+3), resulting in lipid peroxidation and direct toxicity, mainly to the proximal tubular epithelial cells and causes inhibition of the nitric oxide synthesis leading to renal vasoconstriction.3,5,6 This triad of renal vasoconstriction, tubular obstruction and apoptosis causes myoglobin toxicity. However, due to multifactorial aetiology, the role of other concomitant factors in rhabdomyolysis cannot be ignored.
Major aetiologies causing MCN were compared with other studies from India and western countries are enumerated in Table 2. The comparative analysis between etiologic groups in various studies revealed snake envenomation and heat stroke as major cause in Indian Scenarios compared to drug administration and ingestion as major etioloy in western countries. In our study, eighteen patients (72%) gave history of unaccustomed strenuous physical excretion in hot and humid climate of western india. In a study by Knochel et al, it was observed that incidence of exertional rhabdomyolysis was significantly higher in patients who are not accustomed to strenuous exercise like physicians and students and hence, term ‘white collar rhabdomyolysis’ was coined.7 Exertional rhabdomyolysis is more common than traumatic rhabdomyolysis and usually occurs due to continuous muscle contractions compromising capillary blood flow.8
In our study, six patients (24%) gave history of infection and sepsis including dengue fever. In one retrospective study, 6% of the myoglobin cast nephropathy cases were due to infection.3,4 Another study reported that in dengue patients, rhabdomyolysis led to AKI in 15.6─35.8 % of cases with the mortality rate of up to 11.1 %.9 The proposed mechanism for development of infection induced rhabdomyolysis may be multifactorial including tissue hypoxia secondary to sepsis or dehydration, toxin release, associated fever, direct bacterial invasion of muscle, cytokine mediated inflammatory response and tumour necrosis factor alpha (TNF-a).9,10
In our study, one patient (4%) gave history of snake envenomation. Snake venom is composed of enzymes like phospholipase A2 which causes severe skeletal muscle injury leading to rhabdomyolysis.11
Rhabdomyolysis usually presents with classic triad of muscle pain, oliguria, and dark coloured urine. in our study, oliguria was seen in 84% patients while muscle cramps and cola coloured urine was seen in 76% and 56 % cases respectively. Myoglobinuria, (urine myoglobin more than 60 µg/ml) is usually detected by urine dipstick tests (orthotoluidine) which has low specificity due to cross rection with haemoglobin rich red blood cells or haemolysis. In one study, myoglobinuria was positive only in 42% of our patients by dipstick test.5,11
Serum CPK is a sensitive marker and usually increases to more than 5 times the following muscle injury within 12 hours and reaches baseline in 3 to 5 days. This wide variation of serum CPK levels in our study (range 975-7150) were seen probably because over a period, their levels returned to normal by the time the patient developed AKI.4,5,10,11
Myoglobin has a lesser diagnostic value than CPK for detecting rhabdomyolysis because of its small half-life (2-6 hours) and quick return to normal level within 8 hours.
In Rhabdomyolysis, Electrolyte abnormalities usually determine the severity of AKI because they may precede the acute kidney injury. Most common electrolyte abnormalities include hyperkalaemia, hyperphosphatemia, hyperuricemia, high anion-gap metabolic acidosis, and in renal failure cases, hypermagnesemia. Among these, Hyperkalaemia is an early rapidly progressive life-threatening manifestation of rhabdomyolysis.1,4,5,10–12
On Light microscopy, Renal biopsy shows features of acute tubular injury (ATI) with attenuation of tubular epithelial cells, cytoplasmic vacuoles, brush border loss and sloughed out intratubular epithelial cells.3,4,13
According to one study, other associated finding may be of arterial sclerosis and deposition of calcium oxalate.3 Myoglobin casts are usually appeared eosinophilic to brown granular in H&E stain, are weakly PAS positive and fuchsinophilic in MT stain. Differential diagnosis of Myoglobin casts includes other pigment casts like haemoglobin casts and bile casts.5,11–13
As there are no morphological characteristics to differentiate between them, specific IHC for myoglobin and haemoglobin are required as they do not cross react with any other casts. Bile casts are yellow-brown, stain positive (dark green) with Hall stain and usually occurs when serum bilirubin is very high (>20 mg/dL).4,13
Treatment options for MCN includes early and aggressive repletion of fluids (usually >10L/day) with the amount administered depending on the severity of the rhabdomyolysis, preservation of renal perfusion and prevention of myoglobin cast formation. Adjunct therapies, such as urine alkalinization with sodium bicarbonate or 0.45% saline solution and renal replacement therapy, can be lifesaving in severe cases. The advantages of alkalinization include prevention of precipitation of the Uromodulin (Tamm Horsfall protein)–myoglobin complex and inhibition of redox cycling of myoglobin and lipid peroxidation. The only disadvantage of alkalinization is the reduction in ionized calcium, causing exacerbation initial hypercalcaemic phase. The use of diuretics like Mannitol remains controversial while the use of antioxidants and free-radical scavengers like Vitamin E and C may be justified as supportive therapy.4–8,11–15
Prognosis of myoglobinuric AKI is usually good. In our study, 64% of AKI patients required haemodialysis and in 88% patients, renal function returned to normal with full recovery. However, 12% patients succumbed to their illness due to widespread sepsis and multi organ dysfunction syndrome. In comparison, in one study, only 45% of the patients had full recovery while 18% of the patients died, possibly due to underlying disease.3 In a series done on 46 patients,97.8% required haemodialysis, 6.5% died of sepsis/disseminated intravascular coagulation and 12% proceeded to chronic kidney disease (CKD).6 In another study, the mortality rate due to rhabdomyolysis-associated AKI was around 15.4%.12
The better prognosis in our patients could be probably because they were young without associated co-morbidities and IHC for myoglobin was used in all suspected cases for early definitive diagnosis.
Future research is focussing on new potential biomarkers including soluble urokinase plasminogen activator receptor, neutrophil gelatinase–associated lipocalin (NGAL) and urinary myoglobin for early prediction of AKI.15 However, their clinical utility remains under investigation.
Our study is limited by the less number and variety of cases. However, we were able to highlight the spectrum of clinical and morphologic findings. Also, this study emphasizes the need for heightened clinical suspicion for MCN in, especially in high-risk scenarios like exertional injuries, drug toxicity, or severe infections and importance of myoglobin immunohistochemistry for definite diagnosis.
5. Conclusion
In conclusion, In AKI patients, Early identification of MCN and multidisciplinary intervention in complex cases involving sepsis or comorbid conditions are crucial to prevent irreversible renal damage and improve patient outcomes. For definitive opinion, immunohistochemistry for myoglobin must be performed for evidence at the foremost. Also, this study stress upon the importance patient awareness, particularly in scenarios involving exercise-induced rhabdomyolysis to prevent recurrence and promote long-term renal health.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
Ethics approval
This study received ethical approval from the IEC committee of the institute. The need for informed consent was waived due to the retrospective nature of the study, and all data was de-identified
Availability of data and material
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authors’ contributions
HK, conceived the study and collected the data. SP performed the statistical analyses. HK and SP cross checked the data, drafted the manuscript, and all authors contributed substantially to its revision.
Acknowledgements
none