1. Introduction
Heart failure with preserved ejection fraction (HFpEF) represents approximately 50% of all heart failure cases and is associated with significant morbidity, frequent hospitalizations, and reduced quality of life.1 Unlike heart failure with reduced ejection fraction (HFrEF), HFpEF is characterized by normal left ventricular ejection fraction alongside impaired diastolic function, elevated filling pressures, and systemic congestion.2,3 Its clinical presentation is often subtle, with symptoms such as fatigue, mild exertional dyspnea, or peripheral edema, which may be misattributed to aging or common comorbidities including obesity, hypertension, and diabetes.4 The increasing prevalence of HFpEF, particularly among the elderly population, underscores the need for early recognition in primary care settings.
Previous studies have highlighted the diagnostic challenges associated with HFpEF and the utility of biomarkers such as B-type natriuretic peptide (BNP) and echocardiography in confirming the diagnosis.5–7 However, there is limited evidence on the implementation of structured early detection strategies in primary care and their impact on patient outcomes.
This report aims to illustrate the early recognition and management of HFpEF in a 70-year-old woman with multiple risk factors, emphasizing the role of vigilant assessment and structured follow-up in a primary care setting.
Early identification of HFpEF is clinically important, as timely intervention including pharmacologic therapy and lifestyle modification can reduce hospitalizations, improve functional status, and enhance quality of life. By presenting this case, we aim to support the integration of evidence-based diagnostic strategies into routine primary care practice and to highlight areas requiring further research.
2. Case Presentation
A 70-year-old woman presented to her primary care clinic with a six-month history of progressively worsening exertional dyspnea. She reported difficulty walking more than 200 meters without developing shortness of breath and mild ankle edema in the evenings. She denied chest pain, palpitations, orthopnea, or paroxysmal nocturnal dyspnea. Past medical history was significant for long-standing hypertension and obesity (BMI 32 kg/m²). She had no history of diabetes, chronic kidney disease, or prior cardiac events. Family history was notable for hypertension and stroke. She was a non-smoker and reported minimal alcohol consumption.
Vital signs on examination included BP 148/86 mmHg, HR 88 bpm, RR 18/min, and O2 sat 97% on room air. Cardiac examination revealed normal S1 and S2, with no murmurs, rubs, or gallops. Lung auscultation demonstrated bibasilar crackles. Mild pitting edema was present in both ankles. The remainder of the examination was unremarkable.
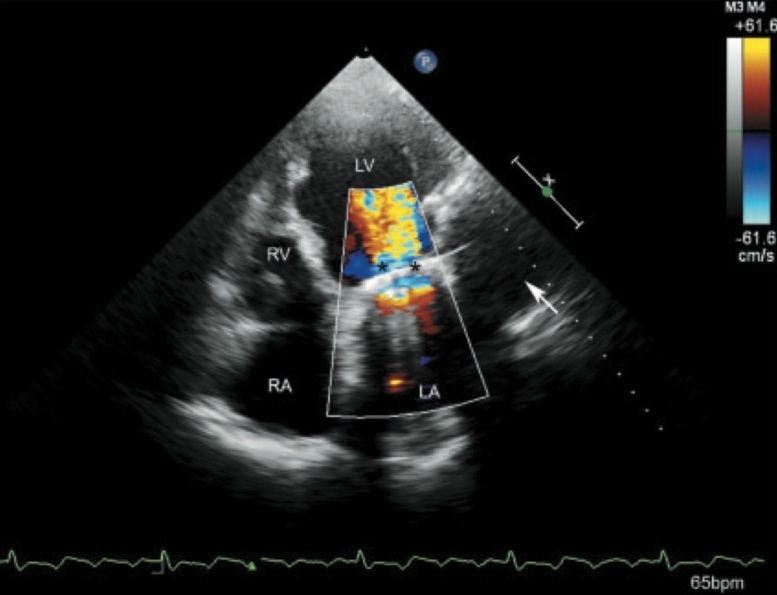
Laboratory investigations showed an elevated BNP of 210 pg/mL. Renal function, electrolytes, and fasting glucose were within normal limits (Table 1). Electrocardiogram revealed sinus rhythm with left ventricular hypertrophy. Transthoracic echocardiography revealed preserved left ventricular ejection fraction (60%), mild concentric left ventricular hypertrophy, left atrial enlargement, and grade II diastolic dysfunction (E/A ratio 1.7, E/e’ 16) (Figure 1).
_showing_mild_concentric_left_ven.jpeg)
The patient was diagnosed with HFpEF based on clinical symptoms, elevated BNP, and echocardiographic findings. Lifestyle modifications were advised, including structured aerobic exercise, sodium restriction (<2 g/day), and gradual weight reduction. Pharmacologic therapy was optimized with continuation of her angiotensin receptor blocker and addition of low-dose loop diuretic.
The patient underwent follow-up assessments at 3, 6, and 12 months. At the 3-month visit, she reported improved exertional tolerance and resolved ankle edema, with BNP reduced to 180 pg/mL. By 6 months, minimal dyspnea was noted, lung sounds were normal, and BNP further decreased to 150 pg/mL. At 12 months, she remained asymptomatic, with normal examination findings and BNP of 120 pg/mL. Functional capacity was maintained through adherence to exercise and pharmacologic therapy (Table 2). Repeat echocardiography at 12 months demonstrated stable structural parameters and diastolic function (Figure 2).
3. Discussion
Heart failure with preserved ejection fraction (HFpEF) is increasingly recognized, particularly among older adults with comorbid conditions such as obesity and hypertension.8 Diagnosis is frequently delayed in primary care because symptoms such as exertional dyspnea and mild peripheral edema are nonspecific and often attributed to aging or coexisting conditions.9 Early recognition is therefore crucial to improve clinical outcomes.
According to contemporary diagnostic frameworks, including the Heart Failure Association Pre-test assessment, Echocardiography and natriuretic Peptide score (HFA-PEFF) and the 2021 European Society of Cardiology (ESC) heart failure guidelines, HFpEF diagnosis requires the presence of heart failure symptoms, preserved left ventricular ejection fraction, elevated natriuretic peptides, and objective evidence of diastolic dysfunction.10,11 In this patient, progressive exertional dyspnea, preserved LVEF (60%), elevated BNP levels, left atrial enlargement, and grade II diastolic dysfunction fulfilled these criteria, allowing a confident diagnosis in the primary care setting.
Measurement of natriuretic peptides and transthoracic echocardiography remains central to HFpEF evaluation. Elevated BNP reflects increased intracardiac filling pressures, while echocardiography provides assessment of diastolic function and structural remodeling.12 In this case, integration of clinical findings with biomarkers and imaging enabled early diagnosis despite a relatively mild initial presentation.
Management focused on optimization of comorbidities and symptom relief through lifestyle modification and guideline-based pharmacologic therapy. Blood pressure control and low-dose diuretics addressed congestion, while angiotensin receptor blocker therapy was continued given the presence of hypertension and left ventricular hypertrophy. Although sodium–glucose cotransporter-2 inhibitors have demonstrated benefit in HfpEF,13,14 they were not initiated due to stable symptoms and an adequate response to initial treatment.
The patient’s sustained clinical improvement and gradual reduction in BNP levels over 12 months highlight the importance of early diagnosis and structured follow-up in primary care. While this report describes a single patient, it aligns with existing primary-care–based studies demonstrating that structured assessment using natriuretic peptides and echocardiography can facilitate early HFpEF detection and reduce symptom burden when combined with regular follow-up.
4. Conclusion
Heart failure with preserved ejection fraction often goes undiagnosed in older adults, especially women who also have obesity and hypertension. This case illustrates that early detection in primary care by a combination of clinical assessment, biomarkers and echocardiography can significantly alter the clinical course. Structured lifestyle adaptation and optimization of pharmacologic management are effective methods at preventing hospitalization, enhancing functional capacity, and decreasing symptom burden. Healthcare providers should have a high index of suspicion for HFpEF in patients presenting with subtle exertional symptoms, and there is a role to incorporate regular follow-up into the primary care setting to achieve sustained effects. Further work is needed to confirm early detection methods and determine long-term outcomes of structured primary care in larger populations.
Ethics approval
Written informed consent was obtained from the patient for publication of this case report.
Availability of data
Data sharing is not applicable as no new data were generated or analyzed.
Competing interests
The authors declare no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors’ contributions
AR drafted the initial manuscript. EAS and GAK contributed to clinical data collection and interpretation. AAF and QBKA contributed to literature review and manuscript preparation. TA supervised the study and critically revised the manuscript. All authors reviewed and approved the final version of the manuscript.
Acknowledgements
None.