1. Introduction
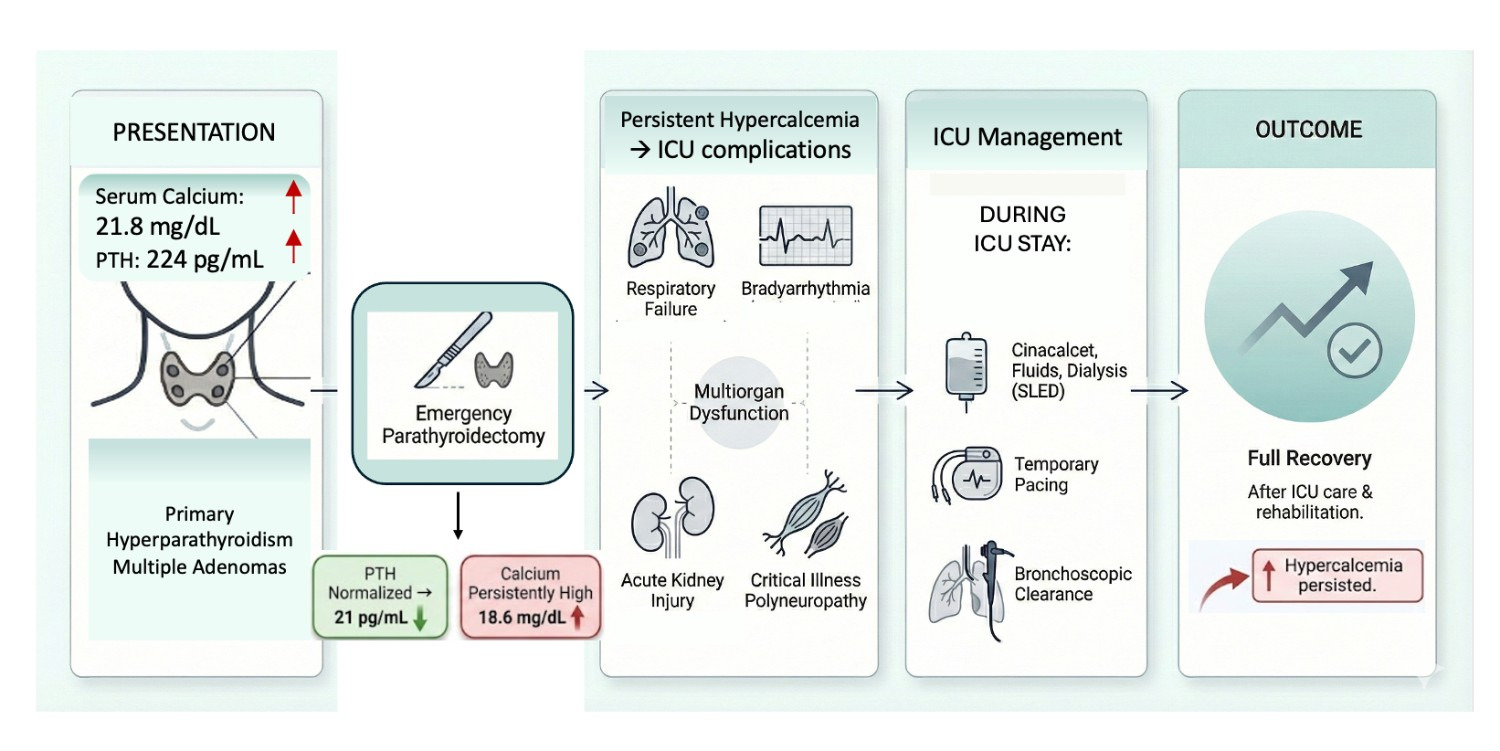
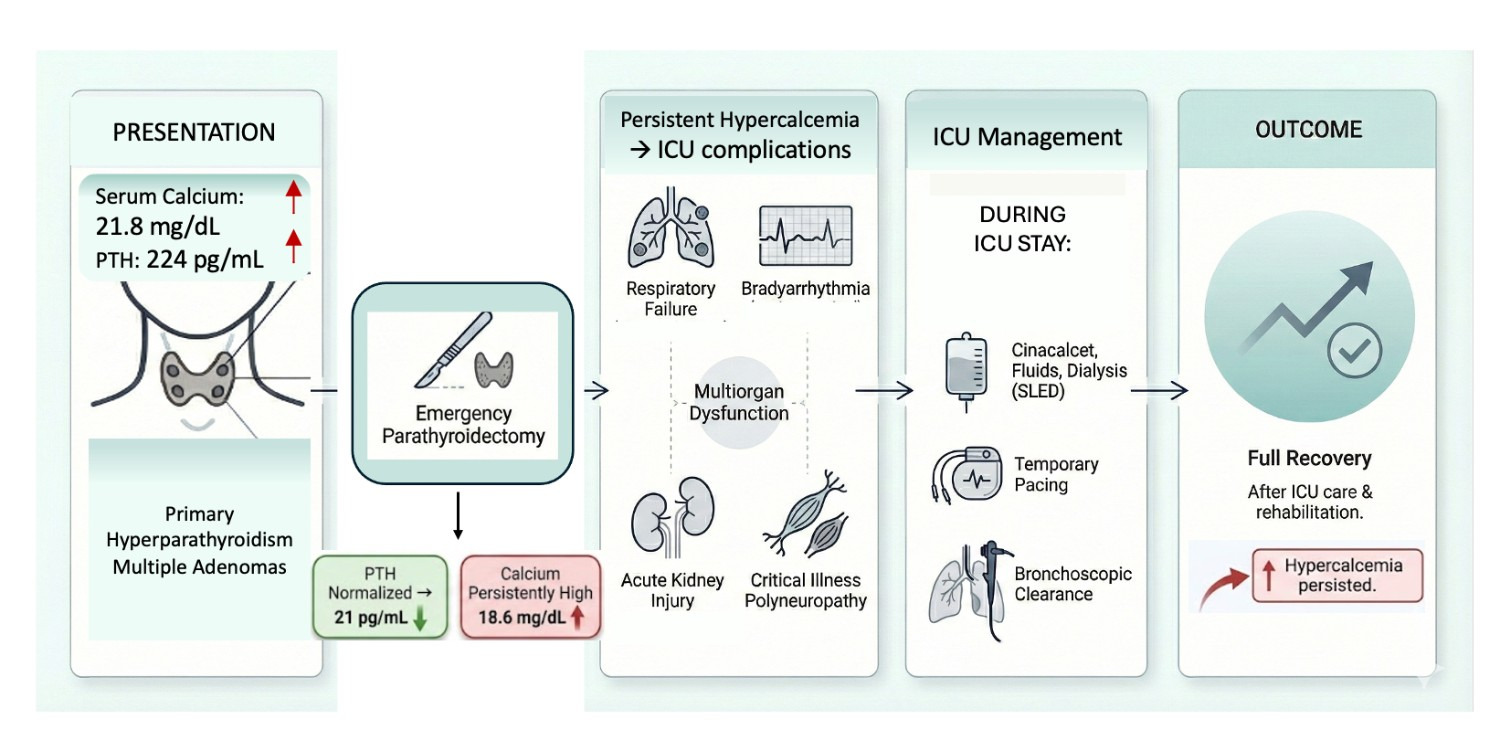
Parathyroid crisis is a rare but life-threatening manifestation of primary hyperparathyroidism characterized by extreme hypercalcaemia and multiorgan dysfunction. Most patients with hyperparathyroidism remain asymptomatic or present with nephrolithiasis or musculoskeletal complaints.1,2 Mortality in parathyroid crisis increases significantly when diagnosis and definitive management are delayed, due to neurological depression, cardiovascular instability, renal failure, and respiratory compromise.3–5 We report a case of parathyroid crisis associated with severe systemic involvement requiring prolonged intensive care and multidisciplinary intervention. Figure 1.
2. Case presentation
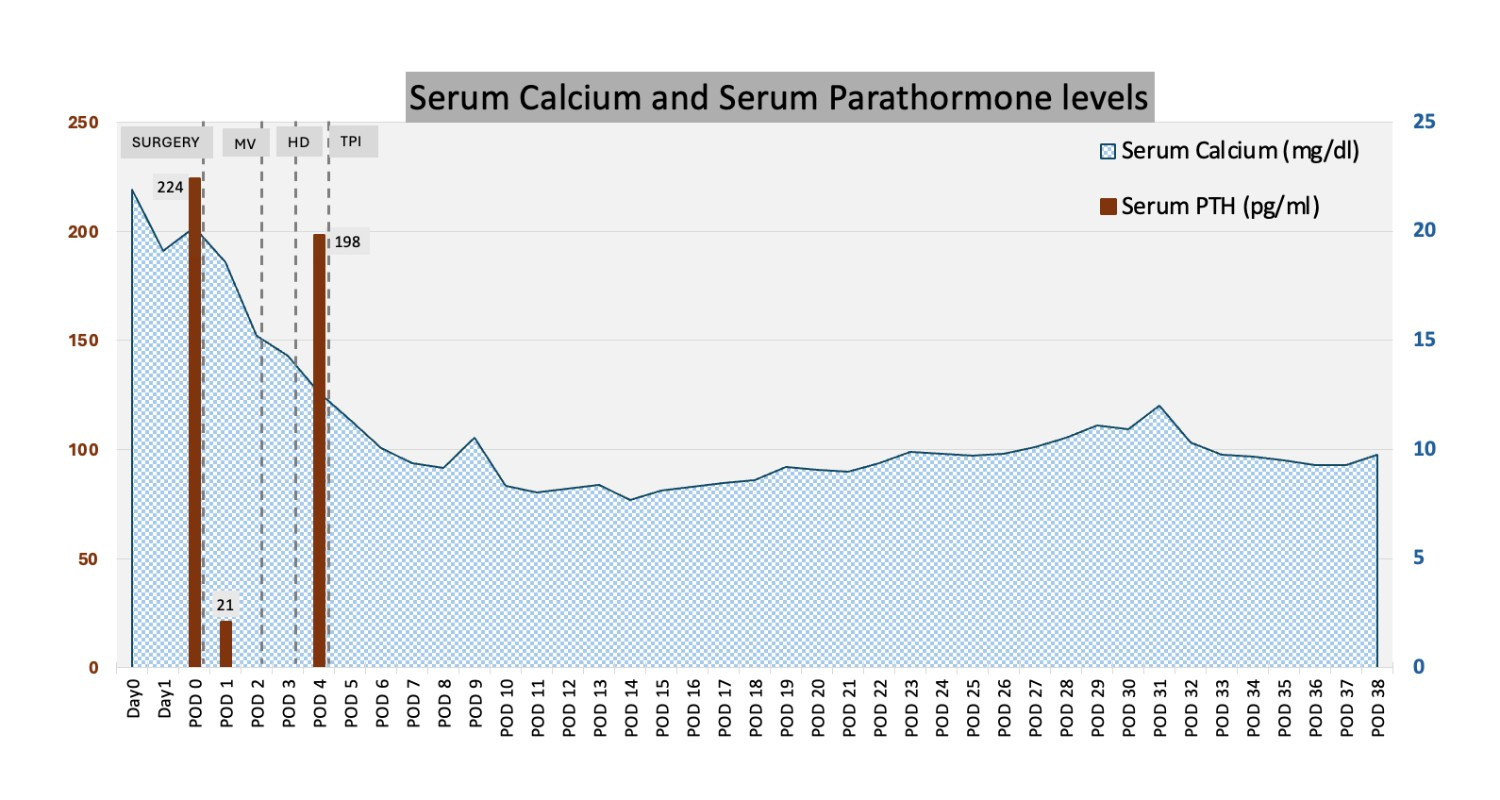
A 52-year-old woman with diabetes mellitus presented with acute-onset vomiting and no prior symptoms suggestive of hypercalcaemia. There was a family history of sudden cardiac death in a sibling. Laboratory evaluation revealed severe hypercalcaemia (corrected calcium 21.8 mg/dL, normal range 8.6-10.6 mg/dL) and markedly elevated parathyroid hormone (PTH) concentration (224 pg/mL; normal: 9–44.6 pg/mL) with normal vitamin D levels (18.5 ng/mL; normal: 20-50 ng/mL), supporting a diagnosis of primary hyperparathyroidism. Contrast-enhanced computed tomography of the neck identified multiple parathyroid adenomas. Table 1.
She underwent emergency excision of three adenomas. The intraoperative period was uneventful; however, she remained obtunded postoperatively with persistently elevated calcium levels. Her serum PTH levels fell to 21 within 24 hours however, serum calcium showed only a marginal fall to 18.6 mg/dL. By 48 hours, she developed hypoxemic respiratory failure necessitating mechanical ventilation. Chest radiography revealed bilateral opacities with collapse of the left lower lobe. She exhibited markedly impaired respiratory mechanics and refractory desaturation, necessitating deep sedation and neuromuscular blockade.
Urgent fibreoptic bronchoscopy revealed diffuse airway inflammation and thick blood-tinged mucus plugs obstructing the left bronchial tree. Repeated bronchoscopic clearance enabled lung expansion and improved oxygenation. Hypercalcaemia persisted during her first week in the intensive care unit (ICU), requiring intravenous normal saline, cinacalcet, and subsequently sustained low-efficiency dialysis to assist calcium clearance and associated oliguric acute kidney injury.
During this period, she developed intermittent sinus bradycardia and recurrent episodes of asystole requiring isoprenaline infusion and subsequent temporary transvenous pacing for seven days. Serum calcium levels eventually normalized with hemodialysis and cinacalcet. Figure 2.
She later developed ventilator-associated pneumonia with sepsis. Initial therapy with intravenous meropenem was escalated to polymyxin B when bronchoalveolar lavage cultures revealed multidrug-resistant Acinetobacter baumannii. Persistent fever and borderline hypotension resolved after minocycline was added.
Despite improvement in respiratory and renal function, she remained encephalopathic and profoundly weak. She demonstrated grade 2 power in the upper limbs, inability to lift her head, and absent deep tendon reflexes. Given asymmetry in weakness, a spinal cord infarct or hypoxic myelopathy was suspected. Magnetic resonance imaging (MRI) of spine was deferred initially due to transvenous pacing but later performed and was unremarkable. Following reduction in generalized oedema, nerve conduction studies confirmed critical illness polyneuropathy attributable to sepsis, systemic inflammation, and paralytic exposure.
Weaning failure necessitated tracheostomy. With gradual ventilatory liberation and intensive physiotherapy, her neuromuscular strength improved steadily.
.png)
2.1. Surveillance
After a month-long ICU stay, she was discharged with normalized calcium levels and kidney function on cinacalcet and continued rehabilitation. At the two-month follow-up, she demonstrated full neurological recovery. However, she remained on cinacalcet and was readmitted with hypercalcaemia at five months postoperative. At the 9-month follow-up, serum corrected calcium dropped to 7.1 mg/dL and serum PTH increased to 216 pg/mL, necessitating admission and short-duration prophylactic oral calcium and calcitriol supplementation. The persistent hypercalcemia and high serum PTH levels, prompted surgical re-exploration of the neck for residual parathyroid gland, which was negative.
She was restarted on cinacalcet for hypercalcemia subsequently, however calcium levels remained high at most instances during outpatient clinic reviews. She had multiple short hospital admissions for normalisation of serum calcium levels interspersed with occasional episodes of hypocalcemia, warranting cessation of cinacalcet and supplementation with calcium and calcitriol supplements. She gradually developed chronic kidney disease with high serum creatinine and phosphorous, likely due to persistent hypercalcemia. On her last follow up visit, her corrected calcium was 16.2 mg/dL for which she was administered calcitonin and intravenous denosumab. She continued endocrinology follow up for 22 months after her first presentation, and subsequently went elsewhere for follow-up. Table 2.
3. Discussion
Parathyroid crisis represents a severe form of primary hyperparathyroidism, frequently precipitated by dehydration, infection, or surgery. Extreme hypercalcaemia, >20mg/dL can result in high mortality due to systemic complications.1,2 Respiratory dysfunction in hypercalcaemia may result from calcium deposition in pulmonary microvasculature or acute respiratory distress syndrome secondary to systemic inflammation. In this case, airway inflammation and obstruction from tenacious mucus plugs compounded respiratory failure, necessitating repeated emergency bronchoscopies for severe hypoxemia. It necessitated neuromuscular blockade predisposing the patient to polyneuromyopathy. Hypercalcaemia can produce bradyarrhythmias and atrioventricular block. Temporary pacing was required until calcium levels normalized, aligning with existing evidence that atrioventricular dysfunction associated with primary hyperparathyroidism can be reversible. The exact mechanism for this is unclear but could be due to due to calcium deposition in the atrioventricular node.6,7
AKI is well described in hypercalcemia and may result from renal vasoconstriction, volume depletion, or calcium deposition. Renal replacement therapy facilitated calcium clearance.
The use of cinacalcet, a calcimimetic agent, helped suppress residual PTH activity and normalize calcium levels, highlighting the importance of ongoing endocrine management even post-surgery. There are several reasons for the persistence of hypercalcemia after parathyroidectomy. Transient hypercalcemia is common after successful surgery and is often normal, with calcium levels typically normalizing within 48–72 hours and most cases resolving within two weeks. Persistent or recurrent hypercalcaemia after surgery is uncommon but clinically challenging phenomenon. Delayed or fluctuating hypercalcaemia months to years later suggests ongoing dysregulation of calcium–PTH physiology. In a single centre study, 9% had persistent postoperative hypercalcemia and 3% required treatment.8–10 The most common causes described are residual hyperfunctioning parathyroid tissue, multiglandular disease, ectopic or supernumerary parathyroid glands. Primary hyperparathyroidism is well recognised to be characterised by reduced sensitivity to extracellular calcium, resulting in an increased set point for PTH secretion. Residual parathyroid gland could harbour similar abnormalities, which over time become unmasked. Other causes such as medications, chronic kidney disease, malignancy or non-PTH-mediated causes were absent in this case.
Weaning and stay in ICU was prolonged because of nosocomial infection and neuromuscular weakness. The patient developed a secondary nosocomial infection, likely precipitated by invasive procedures and immunosuppression associated with systemic inflammation. This case illustrates the vulnerability of patients with severe hypercalcaemia to neuromuscular complications, compounded by paralytic exposure, systemic inflammation, sepsis and extended ICU stay. Although the pattern of weakness was atypical for critical illness polyneuromyopathy and suggested a potential spinal pathology with a worse prognosis, MRI evaluation could not be undertaken due to cardiovascular instability. This posed a challenging situation for both the treating team and the family, particularly because of the financial burden imposed by the prolonged ICU course.
Extreme hypercalcaemia in parathyroid crisis poses a high risk of multisystem injury. Postoperative metabolic optimisation and coordinated multidisciplinary care after emergency parathyroidectomy is crucial for survival. Early intervention and sustained rehabilitation can result in full recovery, even in complex presentations. This case demonstrates the need for vigilant perioperative and prolonged monitoring for persistently high serum calcium and PTH levels.
4. Key Points
-
Severe hypercalcemia (>20 mg/dL) can lead to life-threatening multi-organ dysfunction, including acute kidney injury, respiratory failure, and bradyarrhythmia.
-
Emergency parathyroidectomy is often required but must be followed by vigilant serum calcium monitoring.
-
Respiratory failure can be multifactorial and severe.
-
Multidisciplinary ICU care with aggressive multiorgan support and continued endocrine management is key to survival and recovery.
Ethics approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Availability of data and material
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
Authors’ contributions
MM and JC conceived the study. MM and PS collected the data. JC cross checked the data. MM, PS, and JC drafted the manuscript, and all authors contributed substantially to its revision.
Acknowledgements
None