Introduction
Superficial dorsal penile vein thrombophlebitis is a benign condition characterized by a palpable, cord-like induration along the dorsal penile shaft, often painful and more prominent during erection.1 It represents the penile form of Mondor’s disease, which was originally described in 1939 as a sclerosing superficial thrombophlebitis of the subcutaneous veins of the anterolateral thoracoabdominal wall.2 Although the clinical course is generally favorable, patients may present with marked distress and fear of malignancy or sexual dysfunction.1 This entity remains mainly described in case reports and small series.1,3
Case presentation
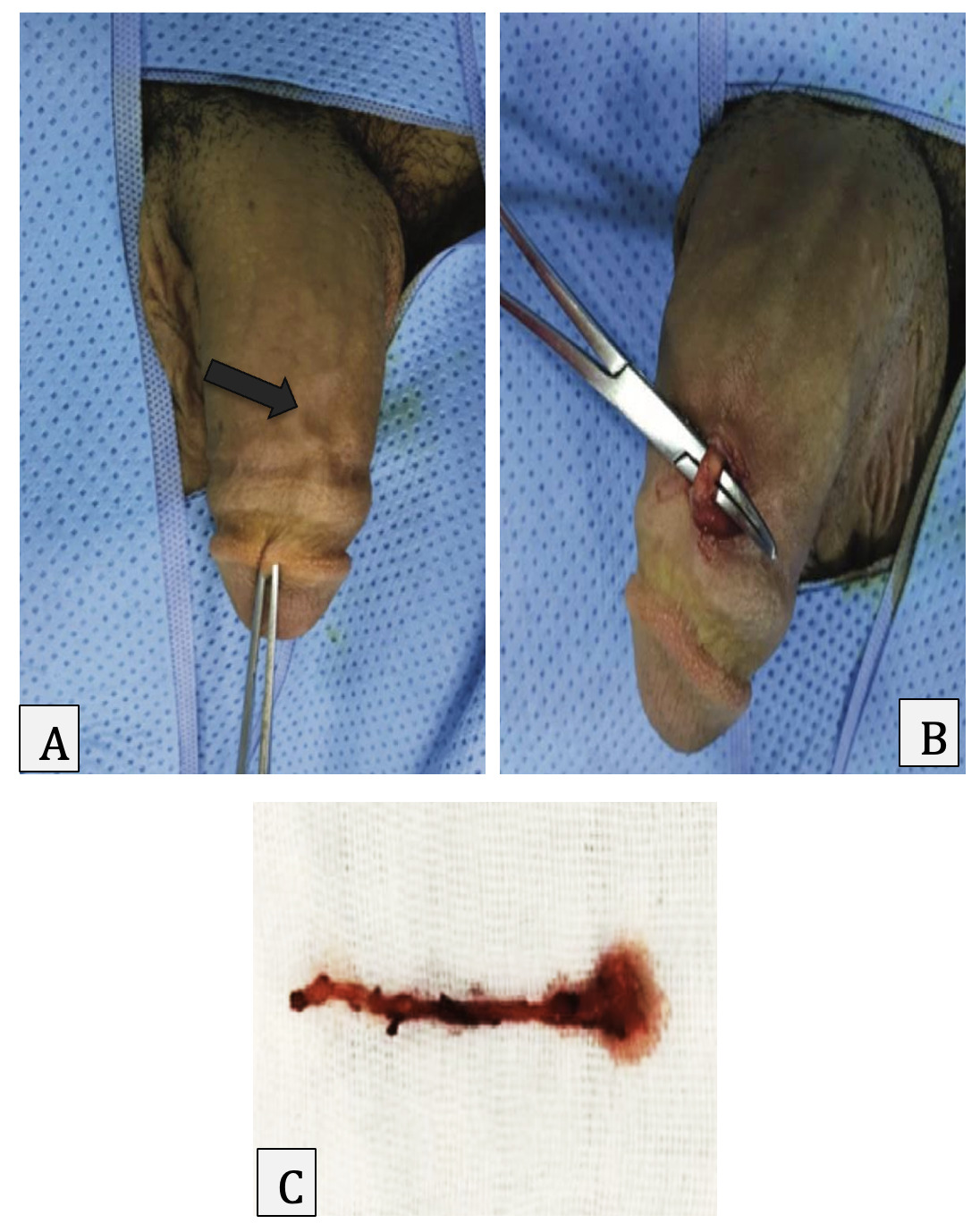
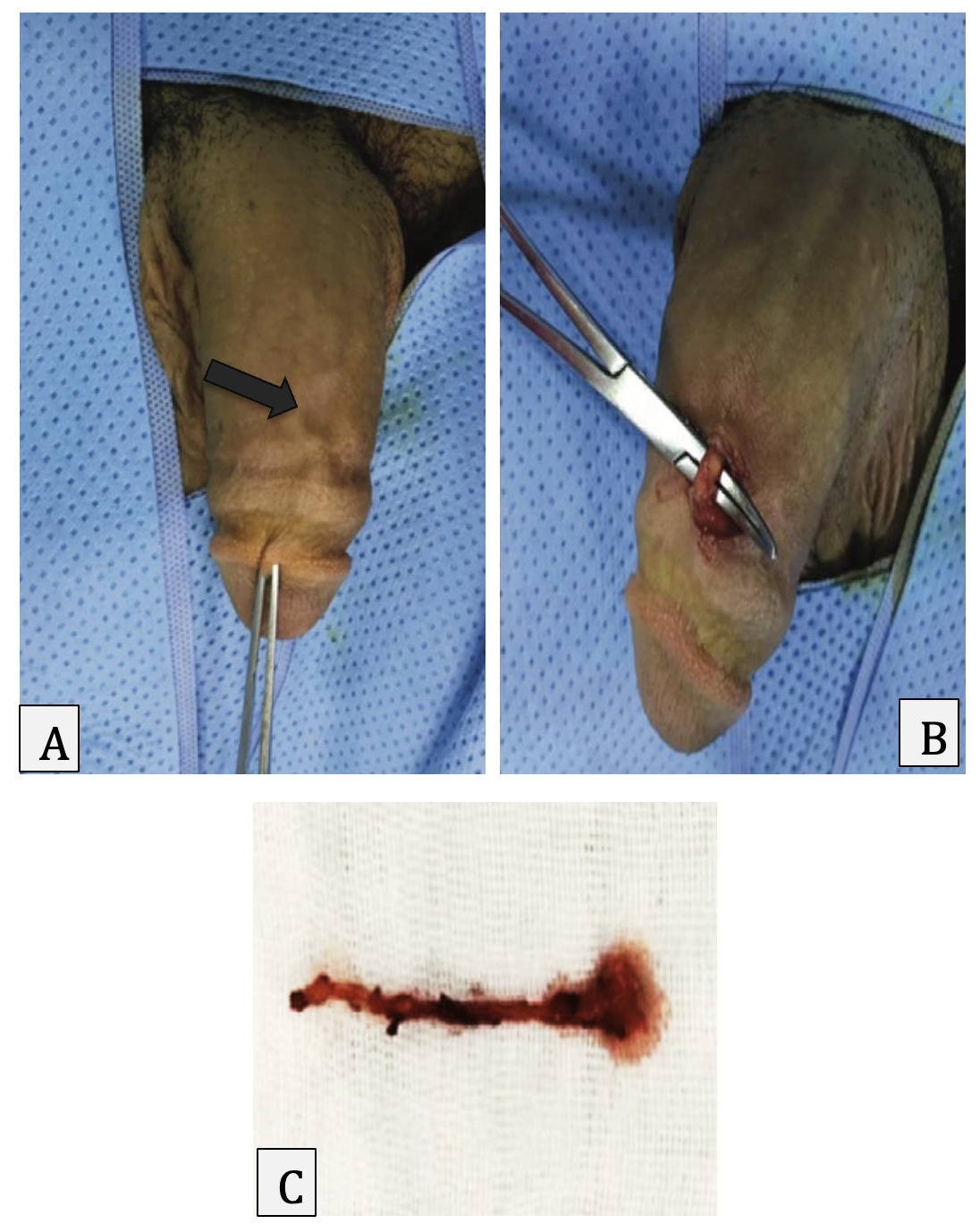
A 37-year-old single man with no notable medical history reported redness and swelling of the penis after sexual intercourse three years before presentation. The inflammatory symptoms regressed incompletely, leaving a persistent sclerotic cord along the dorsal aspect of the penis (Figure 1-A), associated with pain during erection. Clinical findings were consistent with chronic superficial dorsal venous involvement.
Doppler ultrasound was not performed because the clinical presentation was typical and the lesion was clearly localized on examination; the primary goal of intervention was symptom relief after prolonged persistence.
Conservative management options were reviewed with the patient (reassurance, temporary sexual abstinence, and non-steroidal anti-inflammatory drugs). Given the three-year persistence of symptoms with erection-related pain affecting function, the case was considered refractory to expectant management and the patient elected surgical treatment. At exploration, the palpable cord corresponded to an indurated segment of the superficial dorsal penile vein (Figure 1-A). The affected venous segment was dissected and excised (Figure 1-B), and the specimen demonstrated a fibrotic cord-like appearance grossly (Figure 1-C). Histopathological examination demonstrated focal intimal thickening of the venous wall without vascular lumen obstruction and without an identifiable residual thrombus.
The postoperative course was uncomplicated. At 6 months follow-up, the patient reported resolution of erection-related pain and no recurrence of the dorsal cord.
Discussion
This condition is considered rare and is mainly described in case reports and small series.1,3 In retrospective cohorts, the median time to clinical resolution is typically within a few weeks, with a high overall resolution rate.4 The true incidence is likely higher because many cases resolve spontaneously without medical consultation.1,5
Penile venous drainage is commonly described as superficial (subcutaneous) and deep systems. This condition involves the superficial dorsal venous network.1 Thrombosis of the deep dorsal vein represents a different condition that may require urgent assessment.1
Local mechanical trauma (vigorous or prolonged sexual activity or masturbation) is the most frequently reported trigger.1,4 Other suggested factors include prolonged sexual abstinence, penile/pelvic surgery, local or systemic infection/inflammation, intracavernosal injections or vacuum device use, pelvic tumors or paraneoplastic states, and systemic hypercoagulable conditions.1,4 In recurrent or atypical cases, evaluation for thrombophilia and secondary causes may be appropriate.6
Diagnosis is typically clinical: a tender, indurated, cord-like structure along the dorsal penile shaft, sometimes with adherence of the overlying skin.1 Color Doppler ultrasound is the preferred confirmatory test when the diagnosis is uncertain or for follow-up; typical findings include a non-compressible superficial dorsal vein with intraluminal echogenic material and absent venous flow.7
Key differentials are non-venereal sclerosing lymphangitis and Peyronie’s disease.1 Sclerosing lymphangitis usually presents as a serpiginous or annular cord around the coronal sulcus with freely mobile overlying skin and tends to resolve spontaneously; ultrasound does not show venous thrombosis .8 Peyronie’s disease results from fibrotic plaques of the tunica albuginea and is characterized by deformity/curvature rather than a thrombosed superficial vein.1
Conservative management is recommended for most patients: reassurance, sexual abstinence until symptoms resolve, and non-steroidal anti-inflammatory drugs (NSAIDs) for pain and inflammation.1,5 Evidence that medications alter the disease course is limited.1,9 A small prospective series reported clinical and sonographic improvement after 14 days of acetylsalicylic acid plus pentoxifylline ,10 but retrospective data did not demonstrate a clear benefit of adding antiplatelet therapy to common regimens.4
Surgery (thrombectomy or excision of the affected superficial vein) is rarely required but may be considered when symptoms persist beyond the expected recovery window, when a chronic painful fibrotic cord is present, or after failure of conservative therapy.1,11 In our case, the three-year persistence and erectile pain supported surgical management.
Conclusion
Superficial dorsal penile vein thrombophlebitis is a benign condition with a generally favorable prognosis. The diagnosis is usually clinical; Doppler ultrasound is helpful to confirm superficial dorsal vein thrombosis and exclude mimics. Most patients improve with sexual rest, NSAIDs, and reassurance. Surgical excision or thrombectomy is reserved for persistent or refractory cases and can provide symptom relief.
Ethics approval and consent to participate
Ethical approval is not applicable. The case report does not contain any personal information.
Consent for publication
Written informed consent for publication of the clinical details and images was obtained from the patient.
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
Not applicable
Acknowledgements
Not applicable