1) Introduction
Cryptorchidism (undescended testis) is one of the most frequent congenital anomalies in male children. Beyond long-term risks (impaired fertility potential and malignancy), cryptorchid testes are also exposed to acute complications, particularly torsion. Torsion of an undescended testis is uncommon but especially challenging: the absence of typical scrotal findings can mimic other acute conditions (incarcerated hernia, lymphadenitis, appendicitis, or tumor), delaying management and jeopardizing testicular viability.
Through this case report, we aim to emphasize the diagnostic pitfalls and the urgency of management to preserve testicular function when possible and reduce complications.
2) Case report
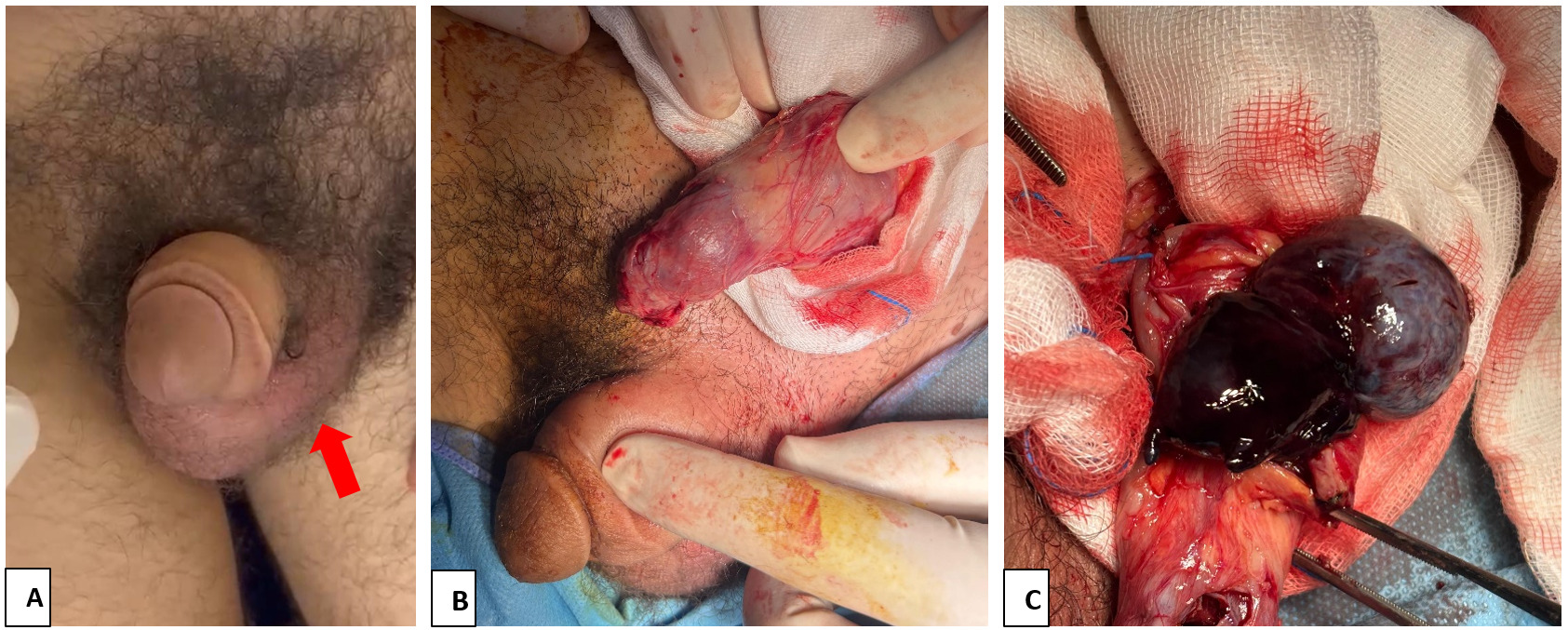
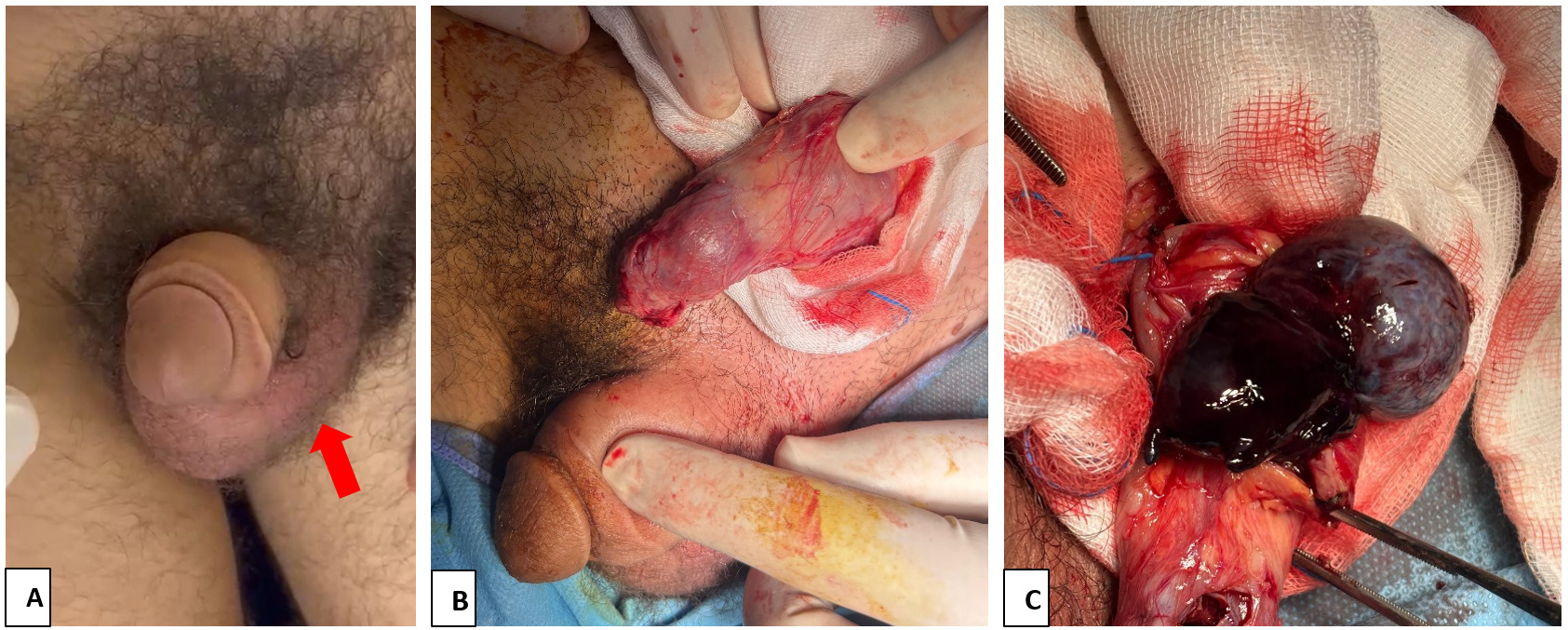
A 16-year-old adolescent with a history of untreated cryptorchidism presented to the emergency department 10 hours after symptom with sudden-onset severe left inguinal pain. He was afebrile and hemodynamically stable, and the general examination revealed no signs of systemic infection. Genitourinary examination showed an empty left hemiscrotum (figure 1-A). A firm, highly tender, non-fluctuant mass was palpable in the left inguinal canal, consistent with an undescended testis, with no overlying erythema or skin changes. The abdominal examination was benign, and there was no history of trauma.
An urgent color Doppler ultrasound demonstrated an intra-inguinal undescended testis with absent intratesticular perfusion, findings strongly suggestive of acute torsion of the spermatic cord in an undescended testis. After obtaining written informed consent from the patient’s parents, the patient underwent inguinal exploration (figure 1-B) 30 min after ED arrival (total ischemia time ~11 hours). Intraoperatively, the spermatic cord was torsed 360°. The testis appeared dark and congested, consistent with advanced ischemia and necrosis (figure 1-C). Detorsion was performed promptly, followed by rewarming with warm saline–soaked gauze for 15 minutes. As the testis failed to reperfuse, it was considered non-viable and a left orchiectomy was performed.A contralateral orchidopexy was carried out during the same procedure to reduce the risk of future torsion.
Postoperatively, recovery was uncomplicated. Pain was controlled with standard analgesia, and there were no early adverse events, including fever, wound infection, hematoma, or urinary complaints. The patient was discharged in good condition on postoperative day 1, with outpatient follow-up arranged. At 1-month follow-up, the postoperative course remained uneventful, with good wound healing and no complications.
3) Discussion
Torsion of an undescended (cryptorchid) testis is an uncommon but highly time-sensitive urological emergency. Unlike the classic “acute scrotum” of torsion in a normally descended testis, cryptorchid torsion frequently presents atypically-most often as acute inguinal or lower abdominal pain with a tender groin mass and an empty hemiscrotum-thereby increasing the risk of misdiagnosis and delayed intervention, with a lower likelihood of testicular salvage.1–3 In our case, the combination of sudden left inguinal pain, an empty left hemiscrotum, and a tender inguinal mass prompted urgent assessment; Doppler ultrasound supported torsion, and immediate exploration confirmed a non-viable torsed undescended testis requiring orchiectomy, with contralateral orchidopexy performed during the same procedure.2,3
Cryptorchidism is one of the most common congenital anomalies in boys and remains clinically relevant in adolescence when orchidopexy has not been performed. Beyond long-term concerns (subfertility and increased malignancy risk), untreated cryptorchidism can lead to acute emergencies such as torsion.4,5International guidelines recommend early referral by 6 months (corrected for gestational age) and orchidopexy ideally between 6 and 12 months and no later than 18 months.4,5 Early orchidopexy facilitates examination and surveillance and addresses long-term risks; this case illustrates the consequences when cryptorchidism persists untreated into adolescence, including preventable emergency presentation and a higher probability of organ loss.4,5
Diagnostic delay is the principal factor associated with poor outcomes in cryptorchid torsion. The presentation may mimic incarcerated inguinal hernia, lymphadenitis, appendicitis (especially right-sided pain), abscess, or even tumor, and the absence of typical scrotal swelling can lead clinicians away from a urological diagnosis.1–3 Therefore, meticulous genital examination is essential in any boy or adolescent presenting with unexplained lower abdominal or inguinal pain. The triad of (i) acute inguinal pain, (ii) a tender inguinal mass, and (iii) an empty ipsilateral hemiscrotum should be considered highly suggestive of torsion of an undescended testis.1,2 In Naouar et al.'s series, symptom duration was substantially shorter in testis-sparing cases than in orchiectomy cases (mean 6.5 hours vs 21.2 hours), emphasizing the impact of delayed recognition and treatment on viability.1
In adolescents with acute groin/lower abdominal pain, always confirm testicular position on exam. An empty hemiscrotum with a tender inguinal mass should prompt urgent urologic consultation and exploration; Doppler can support the diagnosis but should not delay surgery when suspicion is high.
As with scrotal torsion, outcome is time-dependent, and irreversible ischemic injury becomes more likely with increasing duration of torsion and higher degrees of twist.3–6 Even when detorsion allows preservation of the testis, subsequent atrophy can occur, reflecting ischemia-reperfusion injury and incomplete recovery of microvascular perfusion.1,7 Recent pediatric data underline the unfavorable overall salvage in acute cryptorchid torsion: Zvizdic et al. reported a low final salvage rate, and Wang et al. similarly concluded that salvage remains limited and advocated earlier recognition and urgent operative management.8,9 These findings support a “treat as torsion until proven otherwise” approach when clinical suspicion is high.
Color Doppler ultrasound may assist by localizing an undescended testis and demonstrating absent or markedly reduced intratesticular perfusion, thereby increasing diagnostic confidence and helping exclude alternative pathology.2,3 However, ultrasound is operator-dependent and may be limited by pain, bowel gas, body habitus, or difficulty locating a deeply undescended gonad. Consequently, a normal or equivocal Doppler study does not reliably exclude torsion when the clinical presentation is strongly suggestive. In such cases, surgical exploration should not be delayed for further testing.2,3
Surgical exploration is both diagnostic and therapeutic. In palpable inguinal testes, an inguinal approach is standard. Management includes immediate detorsion followed by reassessment of viability after a period of warming/rewarming; if reperfusion occurs, orchidopexy is performed. When the testis remains non-viable despite detorsion and warming, orchiectomy is indicated to avoid retaining necrotic tissue.3–6In our patient, absence of reperfusion after detorsion and warming supported orchiectomy as the appropriate management. An additional consideration in longstanding cryptorchidism is malignancy risk; importantly, tumor and torsion may coexist, and Naouar et al. reported an intraoperative tumor discovered in a patient explored for torsion of an undescended testis.1,4,5Therefore, orchiectomy specimens should be submitted for histopathologic examination, and patients should be counseled regarding surveillance of the remaining testis.4,5
Contralateral orchidopexy is a key preventive step. Predisposing anatomic factors for torsion may be bilateral, and subsequent torsion of the contralateral (remaining) testis can result in catastrophic anorchia. For this reason, prophylactic fixation of the contralateral testis at the time of exploration is widely recommended and carries low morbidity.3–6,8–10 In the present case, contralateral orchidopexy was performed during the same operation, consistent with preventive practice to reduce future torsion risk.
In summary, torsion of an undescended testis should be considered in any boy or adolescent presenting with acute inguinal or lower abdominal pain, particularly when an empty hemiscrotum and a tender inguinal mass are present. Early recognition, avoidance of diagnostic delay, urgent surgical exploration, and contralateral orchidopexy are central to optimizing outcomes. This case also reinforces the importance of timely orchidopexy for cryptorchidism to prevent both long-term risks and avoidable acute emergencies.4,5
4) Conclusion
Torsion of an undescended testis is a rare but organ-threatening emergency with a high risk of delayed diagnosis. Any boy or adolescent with acute inguinal pain and an empty hemiscrotum should be considered to have cryptorchid testicular torsion until proven otherwise. Prompt surgical exploration is essential, and early orchidopexy remains key to preventing avoidable complications.
Ethics approval and consent to participate
Written informed consent was obtained from the patient for the publication of this case report.
Consent for publication
Written informed consent for publication of the clinical details and images was obtained from the patient.
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
Not applicable
Acknowledgements
Not applicable