Patient Presentation
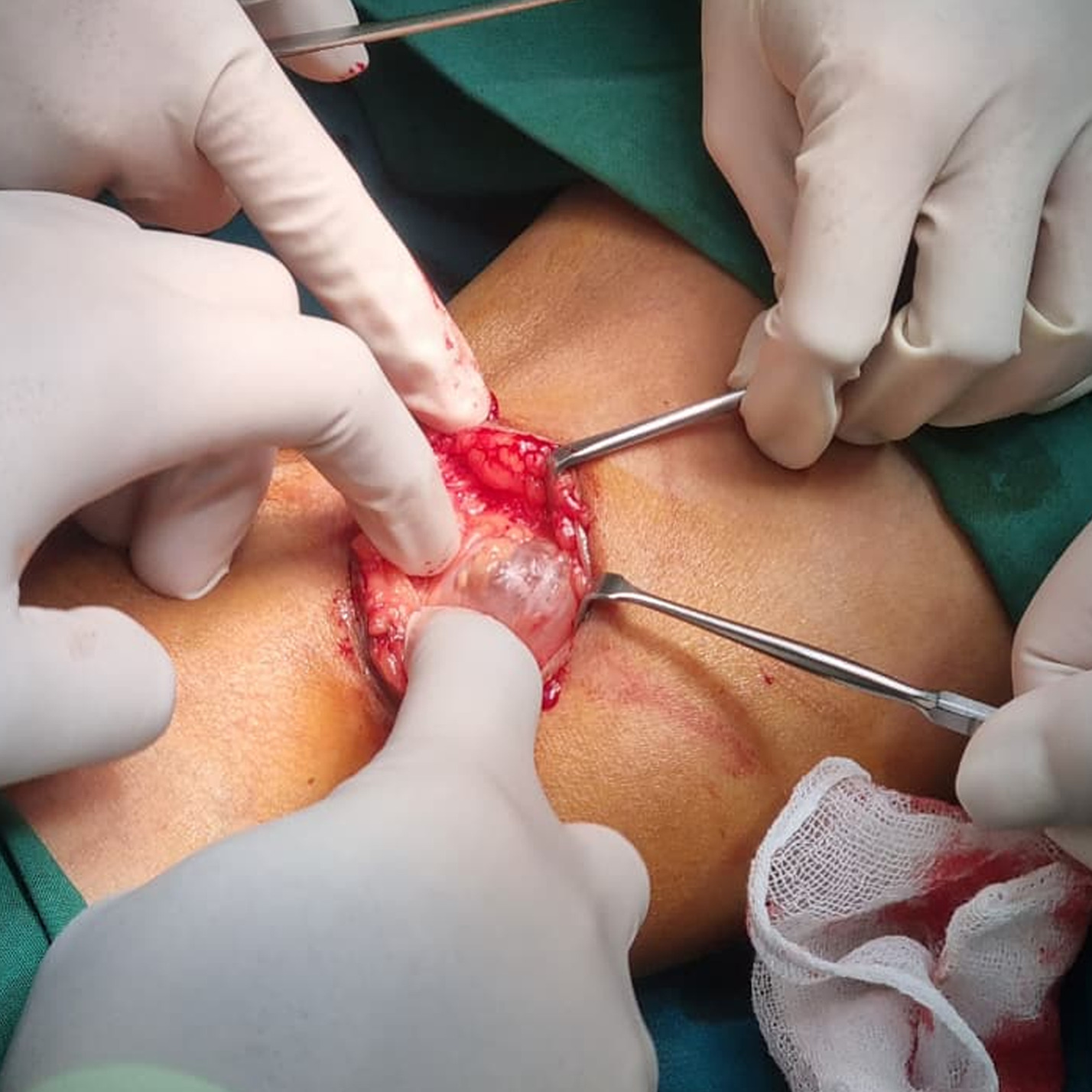
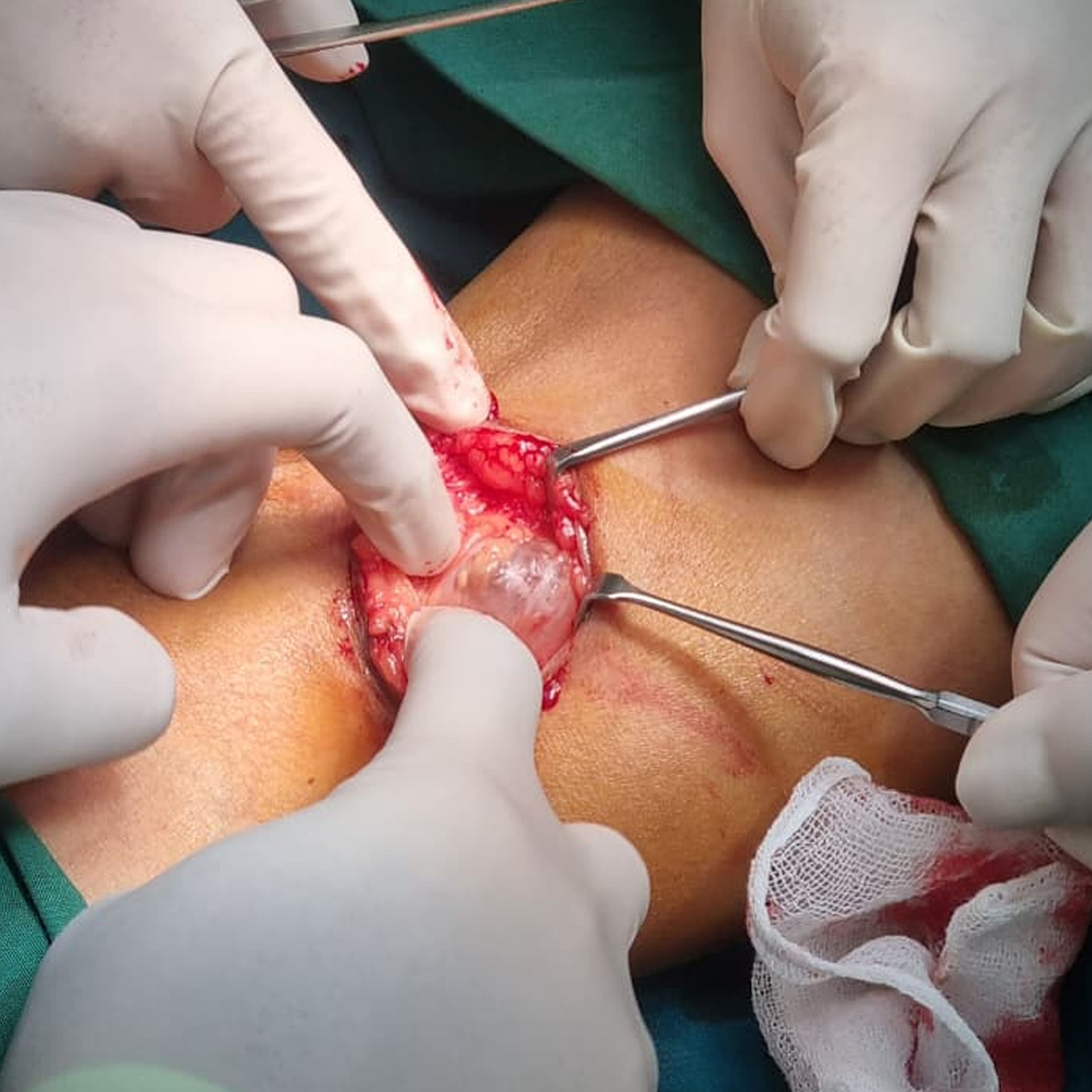
A 54-year-old woman presented with gradually progressive pain and a sensation of fullness in the left knee accompanied by visible posterior knee swelling, exacerbated by walking and knee flexion. She denied a history of trauma or inflammatory joint disease but reported having undergone surgical excision for a similar condition affecting the contralateral knee several years earlier. Physical examination revealed a soft, fluctuant, mobile mass measuring approximately 4 × 4 cm in the left popliteal fossa, with variation in size during knee movement; the lesion was non-tender, without calf edema, and distal neurovascular status was intact. In the absence of red flag features, preoperative imaging was deferred. Surgical excision was performed, and the intraoperative image demonstrated a well-circumscribed cystic lesion arising from the popliteal fossa (figure 1). The patient recovered without immediate postoperative complications.
Diagnosis
Left Baker’s cyst (popliteal cyst).
Discussion
Baker’s cyst is a benign synovial fluid-filled distension of the gastrocnemio-semimembranosus bursa that presents as a posterior knee mass.¹ Clinical features commonly include pain, tightness, or a sensation of fullness, with a palpable mass in the popliteal fossa that may fluctuate with knee flexion and extension.
Diagnosis is often clinical in patients with characteristic findings.1 Important differential diagnoses include deep vein thrombosis, popliteal artery aneurysm, soft-tissue tumors, and abscesses.1,2 Complicated or ruptured Baker’s cysts have been reported to mimic deep vein thrombosis, posing a diagnostic challenge in patients with posterior knee or calf swelling.3 Imaging with ultrasonography or magnetic resonance imaging is recommended when diagnostic uncertainty or red flag features are present, including a pulsatile mass, rapidly enlarging swelling, calf edema, or neurovascular compromise.2 In patients with a typical presentation and intact distal neurovascular examination, imaging may be deferred.
Baker’s cysts are most frequently observed in middle-aged and older adults and are often associated with underlying knee pathology, although they may occur without clinically evident joint disease.1 Management ranges from observation to surgical excision in symptomatic or persistent cases.2 This image highlights the characteristic intraoperative appearance of a Baker’s cyst and reinforces the importance of clinical recognition and risk stratification in patients presenting with posterior knee swelling.