
Introduction
Gynecomastia is defined as the benign proliferation of glandular breast tissue in males and represents the most common breast condition affecting men across all age groups.1 Its prevalence has been reported to range from approximately 30% to 65%, with peak incidence during neonatal life, puberty, and older age.2 Although not life-threatening, gynecomastia is associated with significant psychosocial morbidity. Affected individuals often experience embarrassment, reduced self-esteem, social withdrawal, and symptoms of anxiety or depression.3 In the context of increasing societal emphasis on body image, even mild gynecomastia can result in considerable emotional distress, underscoring the importance of effective management strategies to improve quality of life.4
The ethology of gynecomastia is multifactorial and includes physiological hormonal changes, endocrine disorders, systemic diseases, obesity, medication use, and idiopathic causes, the latter being most common in young, otherwise healthy males.5 While lifestyle modification and medical therapy may be beneficial in early or hormonally active stages, these approaches show limited effectiveness in chronic gynecomastia due to fibrotic tissue changes.6 Consequently, surgical intervention remains the definitive treatment for persistent, symptomatic, or aesthetically concerning cases.7 Surgical techniques for gynecomastia correction have evolved substantially, with the current standard involving liposuction combined with glandular excision.8 The principal variation lies in the incision used to access the gland.9 The peri-areolar incision is widely practiced due to excellent exposure and acceptable scarring, whereas the trans-nipple incision has gained popularity for its minimal visible scar.10 Despite widespread use of both techniques, comparative evidence remains limited. This study aims to prospectively compare peri-areolar and trans-nipple incisions with respect to clinical outcomes, aesthetic results, complications, and patient satisfaction, thereby providing evidence-based guidance for surgical decision-making and patient counselling.
Methods
Study Design and Setting
This study was conducted as a prospective observational study. Patients were allocated to either the peri-areolar incision group or the trans-nipple incision group using a block randomized approach. This prospective, comparative clinical study was conducted at the Department of Burns & Plastic Surgery, Civil Hospital, Ahmedabad, between August 2022 and July 2024. Thirty male patients diagnosed with idiopathic gynecomastia were enrolled and allocated equally into two groups (n = 15 in each): Group A undergoing peri areolar incision and Group B undergoing trans-nipple incision (criss-cross).
Eligibility Criteria
Inclusion Criteria
-
Male patients, age 18–40 years.
-
Idiopathic gynecomastia, clinical Grades I–III (as per Simon classification).
Exclusion Criteria
-
Body Mass Index (BMI) ≥ 30.
-
Pseudo gynecomastia (pure fatty hypertrophy without glandular proliferation).
-
Secondary gynecomastia (e.g., drug-induced, endocrine disorder), significant comorbidities, immunocompromised status (HIV/HBsAg positive), transgender patients.
Preoperative Evaluation
All participants underwent a standardized preoperative work-up including:
-
Detailed clinical history and physical examination, anthropometric measurements (height, weight, BMI).
-
Ultrasound of the breasts to confirm glandular hypertrophy and rule out pseudo gynecomastia.
-
Hormonal profile (as per institutional protocol) to exclude endocrine causes.
-
Standardized preoperative photographs (frontal and oblique) under uniform lighting and patient positioning.
The grade of gynecomastia was classified using the Simon classification for uniformity.11
Surgical Technique
Under general anesthesia, all patients underwent tumescent infiltration using Klein’s solution. Suction-assisted liposuction (SAL) was performed initially to remove adipose tissue and achieve chest contouring. This was followed by glandular excision according to the assigned surgical technique. All procedures were performed by a single senior surgeon to maintain technical consistency and minimize variability related to surgeon experience, thereby ensuring uniformity in operative technique and outcome assessment.
-
Group A: Peri areolar incision at 5–7 o’clock position.
-
Group B: Trans-nipple incision in a criss-cross fashion.
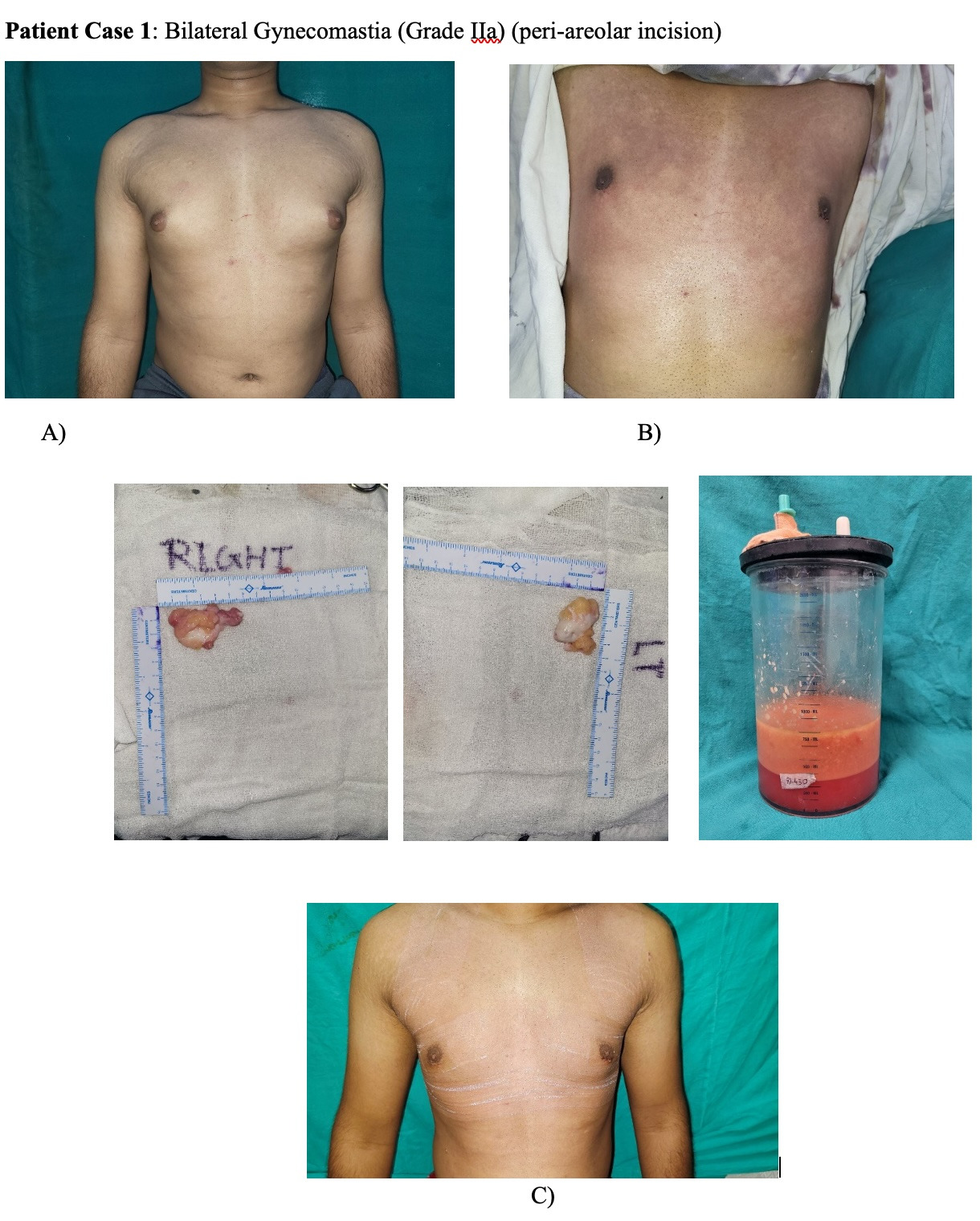
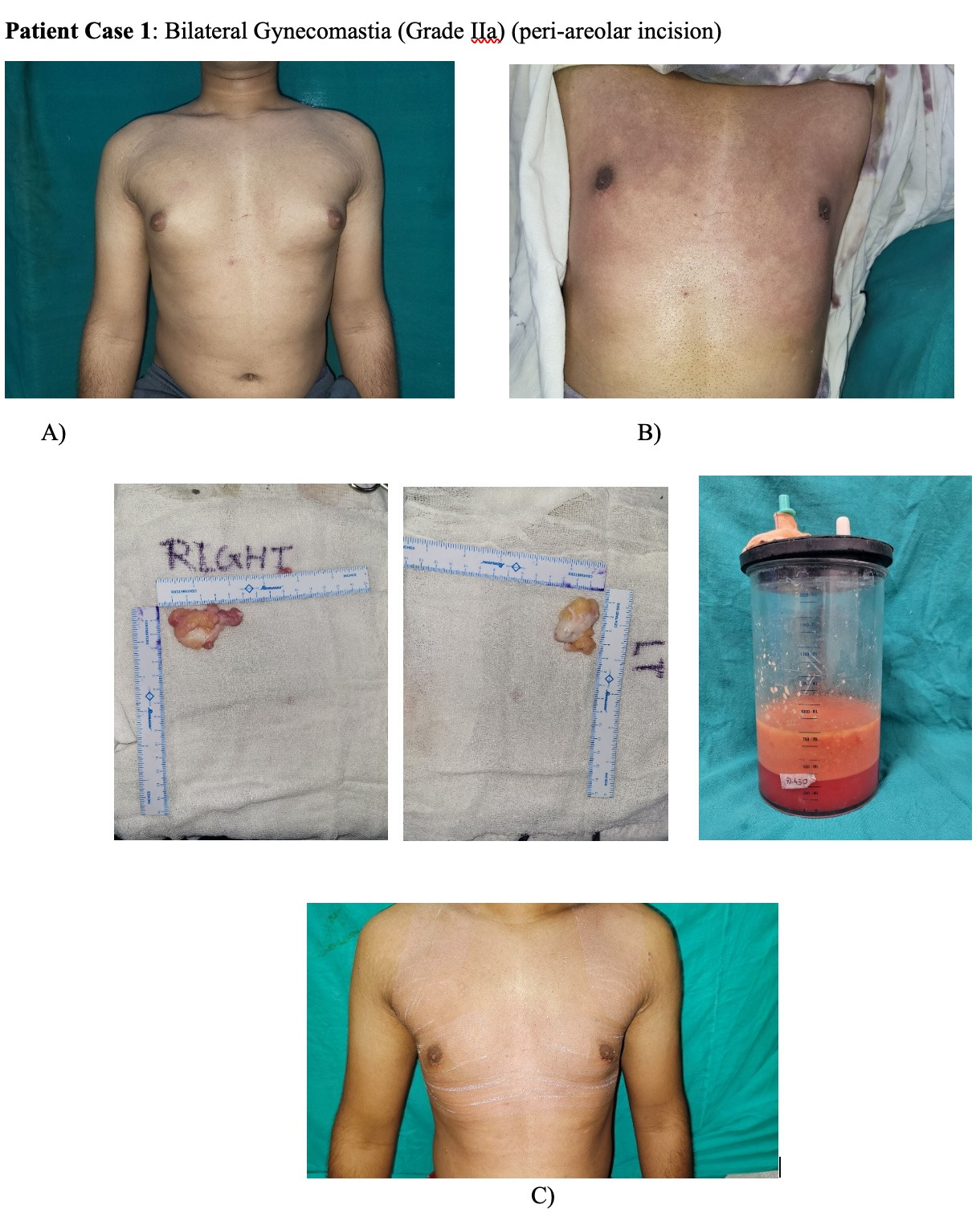
No drains were used in either group. A compression garment was applied immediately postoperatively and advised to be worn continuously for 6 months, except during hygiene.12 Figure 1 depicts a patient’s pre- and postoperative course with Grade IIa gynecomastia.
Outcome Measures
-
Primary Outcome: Patient satisfaction, measured at 6 months postoperatively using a standardized 5-point Likert scale (1 = highly dissatisfied; 5 = highly satisfied).
-
Secondary Outcomes: Operative time (minutes), duration of hospital stay (days), rate and type of complications (e.g., seroma, hematoma, nipple–areola complex necrosis, loss of sensation, contour deformity), and objective aesthetic outcome assessed by independent blinded evaluators (evaluating scar appearance, chest contour symmetry, nipple–areola position) using a predefined scoring system.
Statistical Analysis
A priori power calculation was performed. Assuming a moderate effect size (Cohen’s d ≈ 0.8) for difference in mean satisfaction scores between groups and aiming for 80% power at α = 0.05 (two-tailed), a minimum of 26 patients (13 per group) was required. To account for possible dropouts or loss to follow-up, the sample was expanded to 30 (15 per arm).13
Data were entered into a secured spreadsheet and analyzed using SPSS (version 25.0) and R (version 4.2.0). Continuous variables (e.g., age, BMI, operative time) are expressed as mean ± standard deviation (SD); categorical variables (e.g., presence/absence of complications, satisfaction categories) as frequency and percentage.
The distribution of continuous variables was assessed using the Shapiro–Wilk test. If normality assumption was met, downstream parametric tests were used; if not, non-parametric alternatives were employed.14 For continuous variables with normal distribution, independent samples Student’s t-test was used to compare means between groups. For continuous variables not normally distributed, the Mann–Whitney U test was used.15
For categorical variables (e.g., complication rates, satisfaction categories): Chi-square test or when expected cell counts < 5, Fisher’s exact test.16
To adjust for potential confounding variables (e.g., age, BMI, gynecomastia grade), a multivariate logistic regression model was constructed with the occurrence of any complication (yes/no) as the dependent variable, and incision type, age, BMI, and grade as independent predictors. For continuous outcome (satisfaction score), a multiple linear regression model was used to assess the independent effect of incision technique on satisfaction after adjusting for covariates.
A p-value < 0.05 was considered statistically significant. Confidence intervals (95%) were provided for mean differences and odds ratios (OR) in regression analyses.
Results
A total of 30 male patients were included in the study, with 15 undergoing the periareolar technique and 15 the trans-nipple technique. Baseline demographics were comparable between groups, with a mean age of 25.7 years and average BMI of approximately 23 kg/m², and no statistically significant differences were detected (p = 0.94), confirming group homogeneity.17 Operative parameters demonstrated clear superiority of the periareolar approach, which required significantly less operative time (85 minutes vs 113 minutes; t(28) = 6.14, p < 0.001, Cohen’s d = 2.24), and resulted in a markedly shorter hospital stay (2 vs 6 days; Mann–Whitney U, p < 0.001). Patient satisfaction at 6 months was substantially higher in the periareolar group (4.87 ± 0.35) compared with the trans-nipple group (3.67 ± 1.29), a difference confirmed by both Mann–Whitney analysis (p = 0.002) and ordinal logistic regression, which showed surgical technique as an independent predictor of satisfaction (OR 4.52; 95% CI 1.34–15.21; p = 0.016).18 Complications were significantly more frequent in the trans-nipple group (66.7%) than in the periareolar group (13.3%) (Fisher’s Exact Test, p = 0.003).19 While the periareolar group experienced only seroma in 13.3% of patients, with 86.7% remaining complication-free, the trans-nipple group exhibited NAC necrosis (13.3%), bruising (26.7%), asymmetry (20%), and sensory loss (6.7%), with only 33.3% achieving complication-free recovery.20 Relative risk analysis revealed a five-fold higher risk of any complication in the trans-nipple group (RR = 5.00; CI 1.32–18.9), and contour asymmetry was uniquely present in this group. These findings collectively establish that the periareolar incision offers significantly better clinical outcomes, fewer adverse events, faster recovery, and higher patient satisfaction, confirming it as the safer and more reliable technique for gynecomastia gland excision as given in Table 1. The figures were given in supplementary S1. On subgroup analysis, patients with Grade I and II gynecomastia demonstrated superior aesthetic outcomes and higher satisfaction scores with the peri-areolar incision compared to the trans-nipple approach. In the Grade III gynecomastia cases included in this study, both surgical techniques allowed satisfactory glandular excision. However, limitations related to skin redraping were evident, with a higher incidence of postoperative contour irregularities regardless of the incision approach used. This observation suggests that, in Grade III gynecomastia, surgical outcomes are influenced more by the presence of excess skin than by the choice of incision alone, indicating that incision selection by itself may be insufficient to achieve optimal contour correction in advanced disease.
Transient sensory changes of the nipple areola complex were observed in a small number of patients at the 6-month follow-up, with no cases of complete or permanent sensory loss documented during the study period as shown in Figure 2.

Discussion
The present study provides a comprehensive comparative evaluation of two commonly employed surgical approaches for glandular excision in gynecomastia periareolar incision and trans-nipple incision. The findings clearly demonstrate that the periareolar technique is associated with superior clinical, aesthetic, and patient-reported outcomes when compared with the trans-nipple approach. These results reinforce the established understanding of the anatomical and vascular considerations that govern safe and effective gynecomastia surgery.21
The periareolar incision was shown to offer excellent operative exposure while preserving the integrity of the nipple-areola complex (NAC), resulting in shorter operative times, expedited recovery, and a markedly lower complication profile. The incision follows the natural junction between areolar and surrounding skin, providing both a cosmetically favourable scar and minimal disruption to the subareolar ductal and vascular network. This anatomical advantage likely accounts for the high satisfaction scores observed in our study, alongside the minimal rates of postoperative complications such as necrosis, sensory loss, or contour deformities.22
The favorable outcomes observed with the peri-areolar approach in Grades I and II align with existing literature supporting its reliability in cases with minimal to moderate skin excess. In contrast, Grade III gynecomastia presents unique challenges due to redundant skin and reduced elastic recoil. In such cases, adjunctive skin excision techniques may be required to achieve optimal chest contour, regardless of the gland access incision used. Sensory alterations following gynecomastia surgery are commonly temporary and may continue to improve beyond six months due to progressive nerve regeneration. Therefore, the sensory outcomes reported in this study should be interpreted as intermediate-term findings rather than definitive long-term deficits. Conversely, the trans-nipple incision, although originally proposed as a nearly “scarless” alternative, demonstrated significant drawbacks in the current cohort. The passage of an incision directly through nipple tissue introduces potential compromise of the ductal and vascular systems, thereby increasing susceptibility to complications such as NAC necrosis, bruising, altered sensation, and asymmetry. Indeed, our results showed substantially higher complication rates including a fivefold increased risk of any postoperative complication along with lower patient satisfaction and longer hospital stays. These findings suggest that while the trans-nipple approach may appear advantageous from a scar-hiding perspective, its functional and safety limitations outweigh its theoretical benefits.23
The outcomes observed in this study align closely with previously published evidence. Baumann et al. and Fricke et al. both reported superior cosmetic integration, fewer complications, and predictable glandular exposure with the periareolar approach. Similarly, Holzmer et al. emphasized that the periareolar incision remains the most reliable technique for Grades I and II gynecomastia due to its balance of accessibility and safety. Although the trans-nipple approach has been explored in smaller case series, most of these reports highlight a narrow margin of safety, particularly regarding NAC vascularity and sensory preservation. Our findings reinforce these concerns and add robust prospective data supporting the periareolar approach as the preferred method.24
The advantages of the periareolar incision demonstrated in this study are multifaceted. First, the scar is camouflaged along the natural areolar border, achieving high levels of aesthetic satisfaction. Second, the preservation of NAC vascularity significantly reduces the risk of ischemic complications. Third, the approach offers excellent direct visualization and extraction of dense glandular tissue, which improves operative efficiency and reduces the need for excessive liposuction or blind dissection. Collectively, these strengths contribute to the periareolar approach’s superior safety profile and patient-centered outcomes.25
This study has certain limitations that should be acknowledged. Despite the use of block randomization, some outcome measures were subjective in nature, which may introduce assessment bias. The relatively small sample size and single-center design limit the generalizability of the findings. All procedures were performed by a single senior surgeon, which, while ensuring technical consistency, may introduce operator-dependent bias. The follow-up duration of six months was sufficient to assess early postoperative outcomes and patient satisfaction but may not adequately capture long-term parameters such as scar maturation, late aesthetic changes, and sensory changes of the nipple areola complex. Future multicenter studies with larger cohorts and longer follow-up are required to validate and extend these results.
Conclusion
This prospective comparative study demonstrates that the periareolar incision technique offers significantly superior clinical, aesthetic, and patient-reported outcomes compared with the trans-nipple incision in the surgical management of gynecomastia. Based on the present findings, the peri-areolar approach appears most suitable for Grades I and II gynecomastia, whereas Grade III cases may require additional skin-addressing procedures beyond incision selection alone. The periareolar approach was associated with shorter operative time, faster postoperative recovery, markedly fewer complications, and consistently higher patient satisfaction. In contrast, the trans-nipple technique showed a substantially higher incidence of adverse events including NAC necrosis, bruising, sensory loss, and asymmetry reflecting its inherent risk of ductal and vascular compromise. Given the strong and consistent evidence from this study, the periareolar incision should be considered the preferred and safer technique for gland excision, particularly in Grades I and II gynecomastia. While the trans-nipple approach may offer theoretical cosmetic advantages, its elevated complication rates and reduced predictability limit its clinical utility.
Future studies with larger sample sizes, extended follow-up, and comparison with minimally invasive or endoscopic methods are warranted to further refine surgical practice and enhance long-term outcomes for patients undergoing gynecomastia correction.
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethics Committee in accordance with national and international ethical standards for biomedical research involving human participants (Registration No. ECR/72/INST/GJ/2013/RR-2019). Prior to enrollment, all participants were provided with detailed information regarding the nature and objectives of the study, the procedures involved, potential risks and anticipated benefits, as well as available alternatives. Written informed consent was obtained from each participant before inclusion in the study. Participant confidentiality and data anonymity were strictly maintained throughout the study, and all procedures were conducted in compliance with the principles outlined in the Declaration of Helsinki and relevant regulatory guidelines.
Authors’ Contributions
J.J.M. and N.K. conceptualized and designed the study. S.K.S. was the corresponding author of the manuscript and contributed to data analysis and interpretation and supervised the research. P.M. assisted in data collection and literature review. H.R. contributed to surgical procedures and critical revision of the manuscript. All authors reviewed and approved the final manuscript.
Conflict of Interest
The authors declare no conflicts of interest related to this study.
Acknowledgements
We would like to acknowledge the support of the Department of Burns & Plastic Surgery, B.J. Medical College, Ahmedabad, for providing the necessary infrastructure and resources. We also extend our gratitude to the patients who participated in this study and contributed to the advancement of knowledge in this area.