

Introduction
The cutaneous horn is a conical mass protruding and arising from the skin’s surface. It is composed of cohesive cornified keratotic material originating from basal keratinocytes resembling an animal horn and characterized by a height more than half of the diameter of its base.1
Cutaneous horns appear as projections, usually hard in consistency and non-tender.2 On examination of the horns, they appear as straight or curved outgrowths from the skin that can be white, yellow, or brown in colour but are not limited by these features and can grow in various sizes.3,4 Cutaneous horns can grow from millimetres to centimetres in diameter and are called giant when their height exceeds 1 cm.4 The prevalence of cutaneous horns is unknown as they are rare.5 Cutaneous horns are not only visually unappealing but pose a threat of malignancy requiring surgical intervention.2–6
The first historical documentation of a cutaneous horn case was in 1588 in London of an elderly Welsh female. Her condition was remarkable, and she became a subject of exploitation in circuses and exhibited in pamphlets for profit, and a population with her disease was popular to be known as “horned people”, until the first correct theory was found in the mid-seventeenth century by Danish anatomist Thomas Bartholin who described horns as a tumor tissue arising from the skin.1 The first documented case report with adequate histopathology of gigantic cutaneous horn was reported from Italy. In the late eighteenth century, cutaneous horns were formally recognized as a medical disorder, primarily through the contributions of London surgeon Everard Home and his brother-in-law, John Hunter.7
Case Presentation
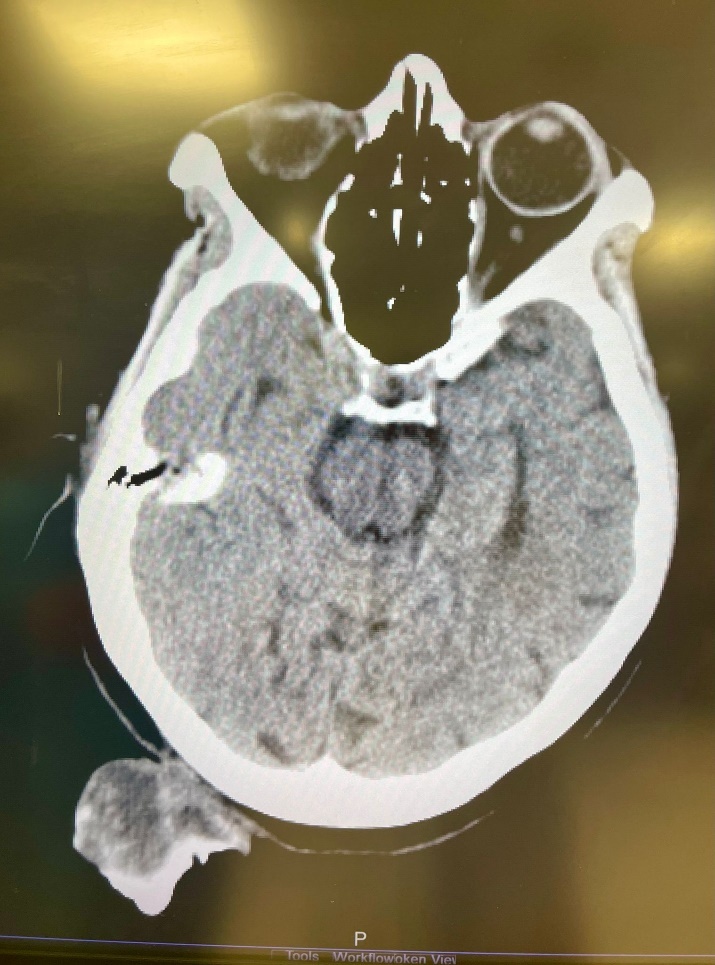
A 75-year-old woman presented to Al Ahli Hospital’s surgery clinic with a painless lesion on the back of her head that had been growing for years. The lesion has grown faster lately, annoying her while lying down and sleeping. The patient is a non-smoker. She had a history of recurrent stasis ulcers on both legs. She had no known drug allergy. Her family history did not include any relevant genetic information or psychosocial history. The physical examination showed a big coiled horn in her occipital area, which measured about 25 centimetres (Fig.1). A Computed tomography (CT) scan revealed a large soft tissue mass arising in the occipital area to the right of the midline with calcification but no bony attachments. The base of the horn is shorter than its length (Fig.2).

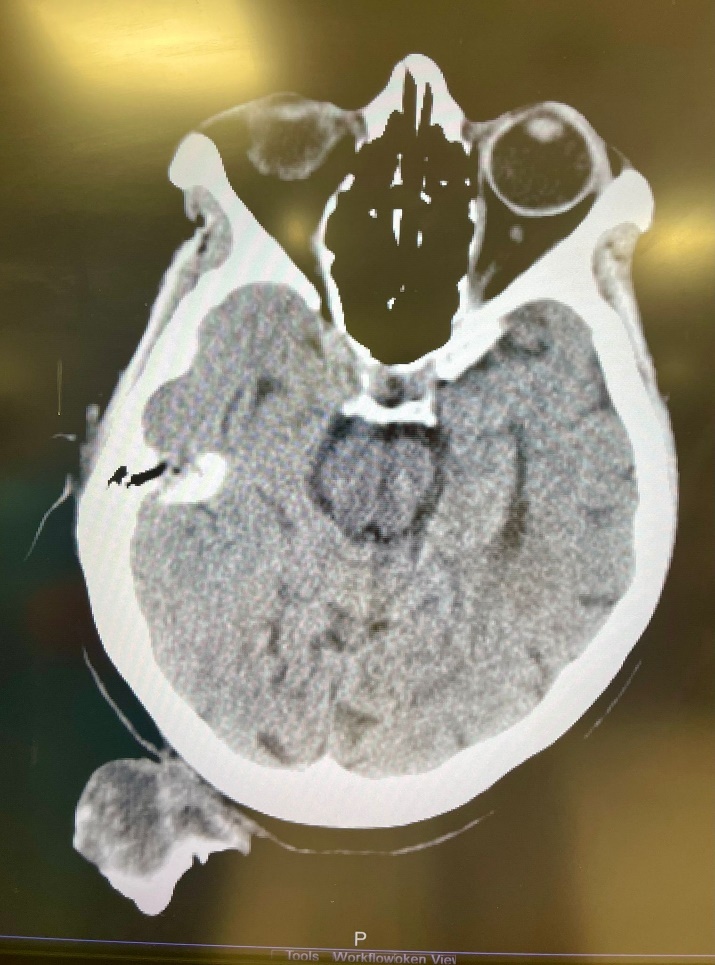
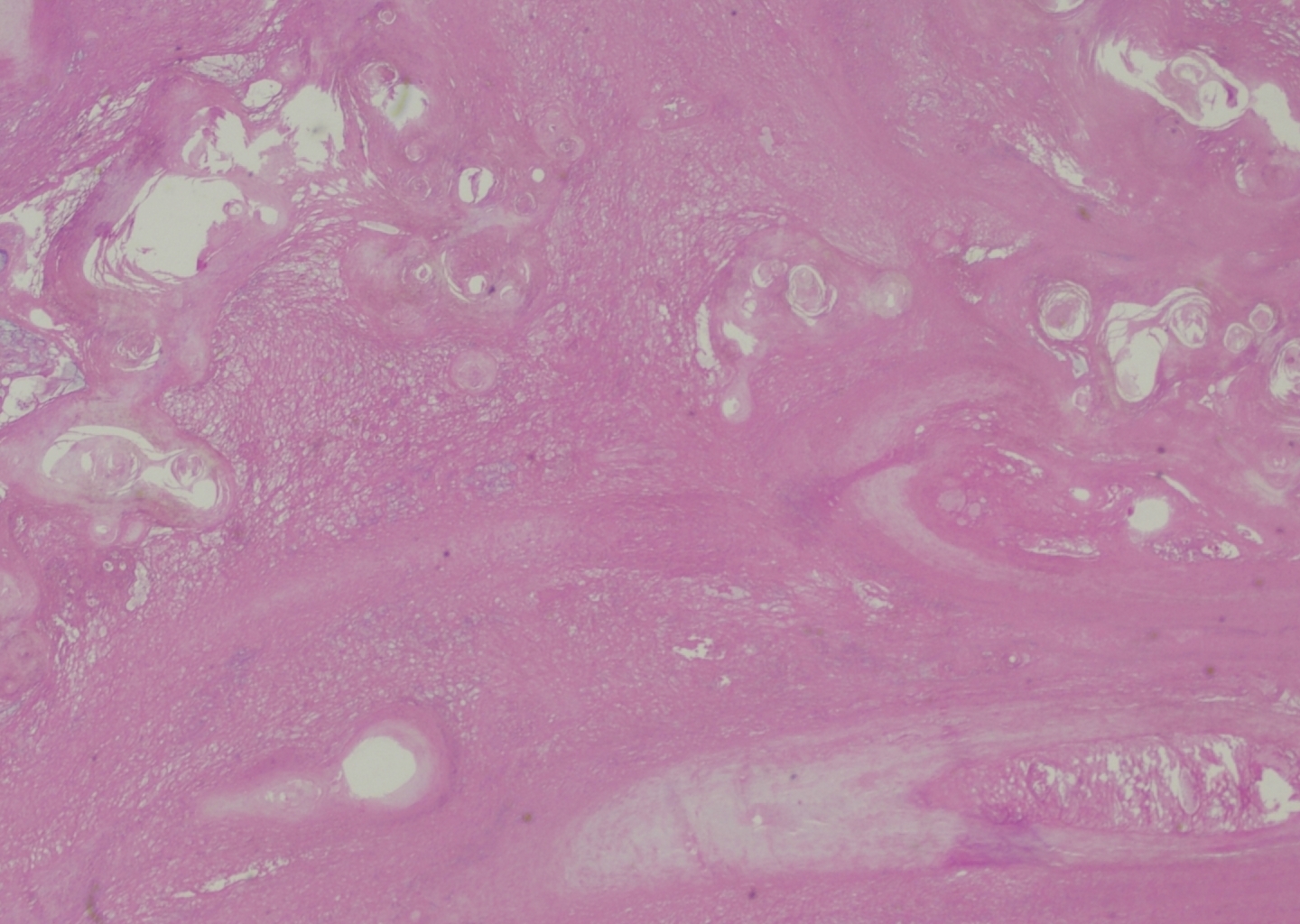
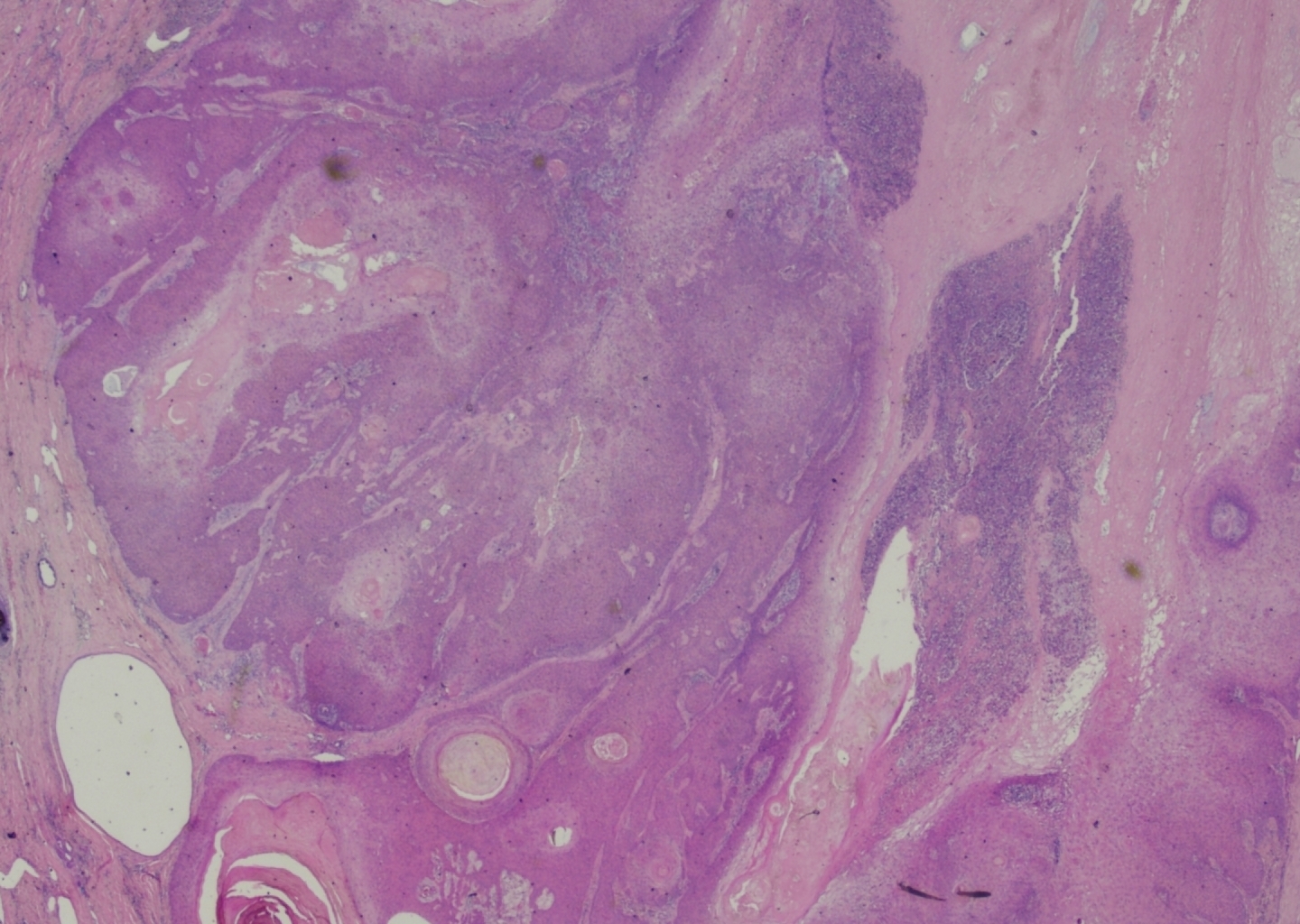
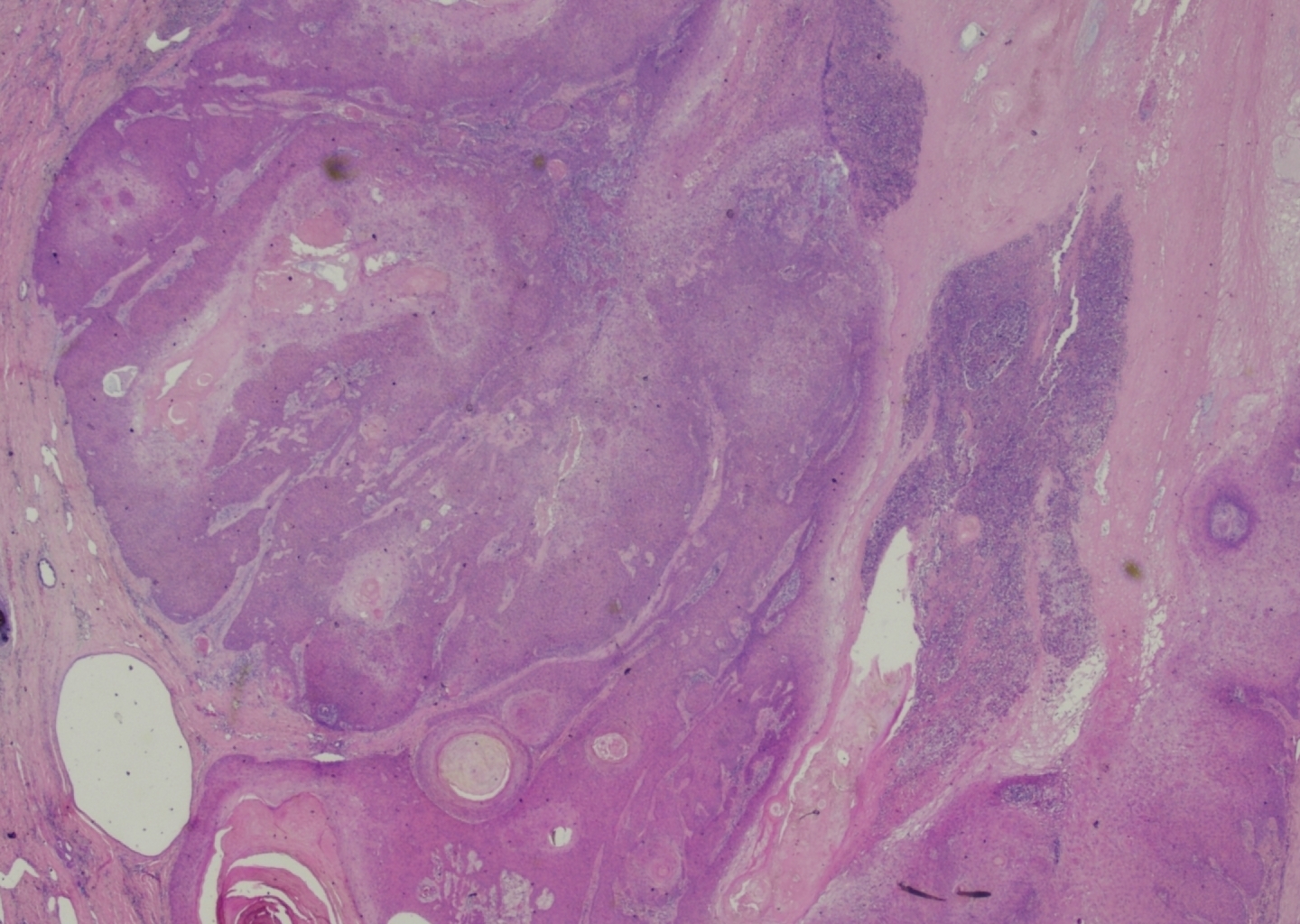
Complete excision of the horn was done with V-Y plasty, and the tissue was sent for pathological examination. A coiled horn measuring 26 cm with an attached skin ellipse measuring 4.5 x 3 cm was received in the pathology laboratory. Histopathological examination revealed a well-differentiated squamous cell carcinoma with keratin horn formation (Figs. 3 and 4). The tumour involves the upper dermis only with no vascular or perineural invasion. The lesion was completely excised with clear excision and deep margins measuring > 4mm. The patient’s surgical excision site healed well (Fig. 5), and there were no clinical recurrences over the 5-year period (the patient was seen at 3, 4, and 5 years after excision).
.jpeg)

Discussion
Cutaneous horns, also known as cornu cutaneum, are hyperkeratotic, exophytic epithelial lesions protruding from the skin resembling animal horns but differing histologically by not having a boney core. They are conical lesions consisting of epidermal keratinocytes develop due to hyperproliferation and hyperkeratosis, with sun exposure being the primary risk factor for their development. Cutaneous horns may arise from a variety of underlying conditions, which can be benign, premalignant, or malignant. The most common benign cause is seborrheic keratosis, followed by lichenoid keratosis. Also, prolonged chronic irritations and infectious causes like Human papillomavirus (HPV) infection have high correlations with their development. Premalignant conditions include actinic keratosis, Bowen’s disease, and arsenical keratosis. Squamous cell carcinoma (SCC) is the most common malignant cause, followed by basal cell carcinoma. Clinically, a height-to-base diameter ratio of one to two and the presence of pain have both been associated with an increased risk of underlying malignancy. In addition, cases of malignant pathology are prevalent in geriatric and light-skinned populations, in males, and sun-exposed areas including head, neck, and upper extremities.1
In a comprehensive study of 643 cases, 38.9% were found to be malignant and 61.1% were benign. Squamous cell carcinoma comprised 94% of all malignant cases of cutaneous horns.8 In the study conducted by Pyne et al., SCC was histologically confirmed as the most prevalent histopathological finding at the base of the horn, accounting for 34.4% (56 out of 163 cases).7 In a large retrospective study of 222 cases of cutaneous horns by Mentese et al., 58.56% of the cases had underlying premalignant and malignant lesions, and 93.7% of the malignant lesions were squamous cell carcinomas in origin.9 The presence of underlying SCC highlights the importance of histopathological examination of cutaneous horns.
A case of a cutaneous horn was reported in a 92-year-old Caucasian female with a posterior scalp giant cutaneous horn measuring 12cm in height and 5.4 cm in base width. The mass was found incidentally, and a computed tomography (CT) scan showed a mass attached to subcutaneous tissues with base calcifications and no bone involvement. Histopathology of the base of the horn showed an invasive squamous cell carcinoma.5
Another case was reported of an 86-year-old white man was found to have a cutaneous horn near his left temple that grew within 6 months. The horn was 6.5 cm in length and 3.5 cm in circumference. The horn was attached to skin and was not causing the patient any symptoms. CT showed no bone involvement, and histology revealed moderately differentiated squamous cell carcinoma keratoacanthomatous features.4 A case of a 28-year-old African female patient came with a cutaneous horn on the temporo-parietal region of the scalp, measuring 3 cm in diameter and 6 cm in height. Histology revealed a verrucoid epidermal hyperplasia. The horn arose from a location of an earlier burn scar.10
A case of cutaneous horn was reported of a 90-year-old female presented with a 9-year history of giant cutaneous horn at her right cheek measuring about 5 cm and associated with squamous cell carcinoma. The patient had a history of actinic keratoses in her face and extremities, and she practiced farm activities that exposed her to the sun for long period of time. This case highlights the risk of long-term sun exposure as a risk for cutaneous horns development. Approximately 30% of cutaneous horns are found on sun-exposed parts such as the upper part of the face and scalp.11
Several case reports have been written on horns. A rare case of a giant horn was reported in a 45-year-old female with a 7-year history of discoid lupus erythematosus (DLE). The patient presented with a brownish-black horn-like lesion in her lower lip, that measured 2.7 × 2.0 cm and developed on a depigmented lesion of DLE. The patient was a non-smoker with no significant sun exposure history, and with good oral hygiene. Histopathological examination showed moderately differentiated SCC superimposing discoid lupus erythematosus (DLE).12
Another case documented from the ophthalmology clinic of a 45-year-old male with a 4-year history of cutaneous horn, 2 cm in height and 1.75 cm in width, in the right lower eyelid. Histopathological examination was consistent with well-differentiated keratinizing squamous cell carcinoma. The authors concluded that histopathological examination is crucial for cutaneous horns, as it was difficult to distinguish clinically between benign, premalignant, and malignant lesions, and complete excision is the recommended treatment.13
Our case underscores that the clinical appearance of cutaneous horns may be misleading, as the underlying lesion can be premalignant or malignant, reinforcing the importance of complete excision and histopathological evaluation of the lesion base, particularly in sun-exposed sites.
Conclusion
In conclusion, this case presents a giant cutaneous horn associated with well-differentiated squamous cell carcinoma, highlighting a notable yet underreported condition. Despite their rarity, cutaneous horns should prompt careful evaluation for potential malignancy, particularly in older patients or those with risk factors. The diagnosis was confirmed through histopathological analysis, which revealed squamous cell carcinoma (SCC) with keratin horn formation, underscoring the importance of thorough investigation. This case reinforces the necessity for proactive management in patients presenting with cutaneous horns, given their potential to conceal underlying malignancies.
Ethical approval
The ethics committee at Al Ahli Hospital, Doha, Qatar, approved this case report.
Sources of funding
This case report received no funding
Statements and Declarations
The authors declare no potential conflict of interest related to this manuscript.
Credit authorship contribution statement
Al-Sulaiti N: Manuscript writing, editing and revision.
AL-Wuhaili A: Manuscript writing, editing and revision.
Alkuwari H: Manuscript writing, editing and revision.
Osman H: Data acquisition and revision.
Al Saady R: Study concept and design, data acquisition, editing and revision