Introduction
Echinococcosis is a zoonotic parasitic disease caused by the larval stage of Echinococcus spp., and is endemic in regions with widespread livestock farming. According to the WHO, it is responsible for approximately 19,000 deaths annually worldwide.1 While the liver and lungs are the most commonly affected organs, pelvic hydatid localizations are exceptionally rare, particularly in the supravesical space.2,3 These atypical presentations may pose significant diagnostic challenges, especially in patients without identifiable risk factors or exposure history. We present a rare case of a supravesical hydatid cyst in an urban patient, highlighting the need to consider hydatid disease in the differential diagnosis of cystic pelvic lesions, even in non-endemic settings.
Case report
A 51-year-old man, with no significant medical history and residing in an urban area, presented with diffuse pelvic pain that had progressed over several weeks. He reported no urinary, digestive, or systemic symptoms.
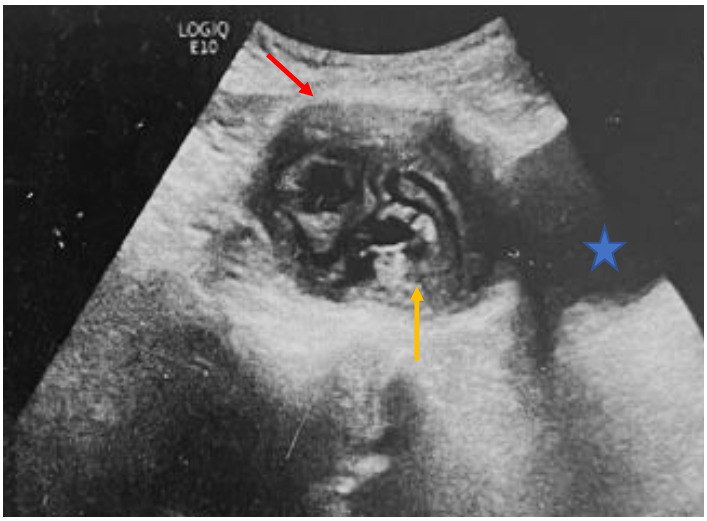
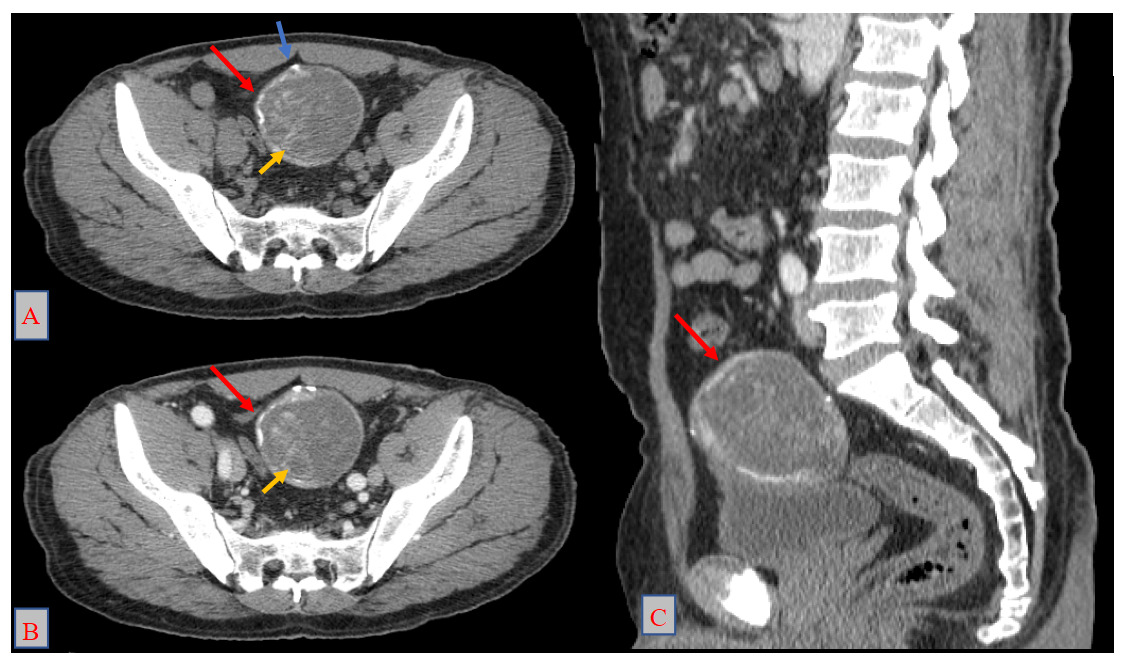
Physical examination was unremarkable. Abdominopelvic ultrasound revealed a supravesical cystic lesion with a thickened wall, classified as Gharbi type III, measuring 53 × 61 mm (Figure 1). Contrast-enhanced CT confirmed a well-defined supravesical cyst, approximately 80 × 60 mm, displacing the bladder inferiorly, with no evidence of adjacent tissue invasion or other hydatid localizations (Figure 2). Serological testing for hydatid disease was positive, further supporting the diagnosis.
_w.png)
_axial_section_before_contrast_injection__(b)_axial_section_after_contr.png)
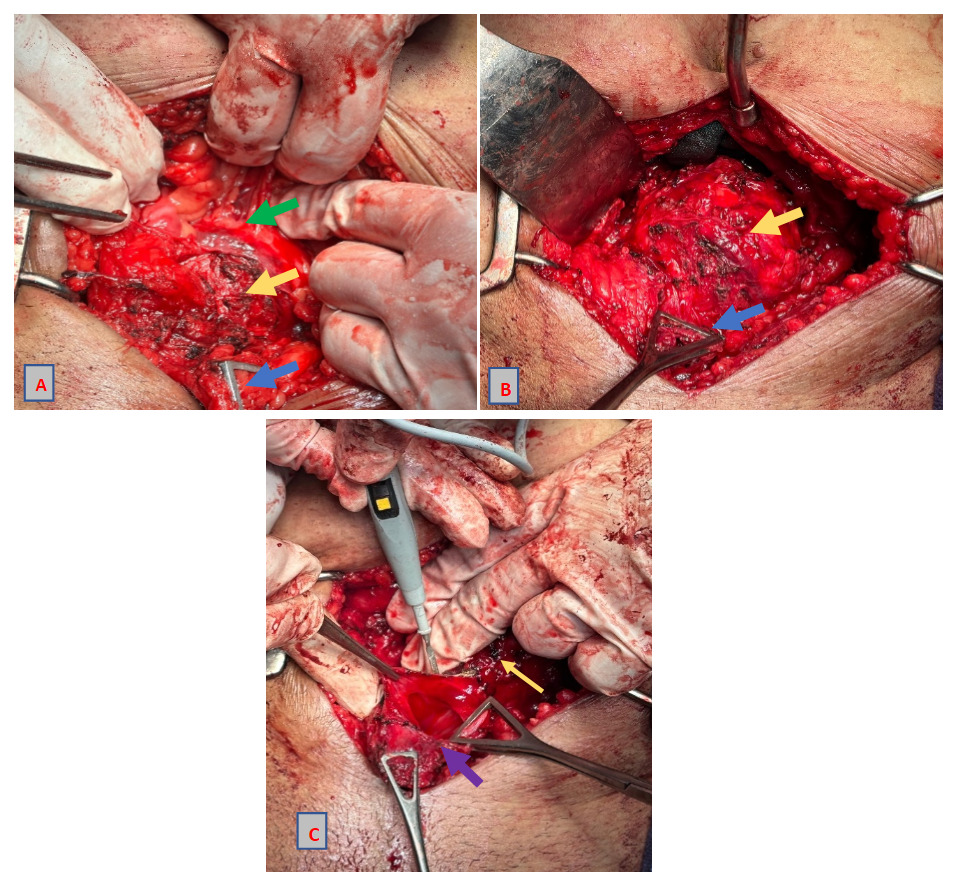
The patient underwent surgical exploration via a midline laparotomy, with subperitoneal access. Due to dense adhesions between the cyst, the pelvic peritoneum, and the bladder dome, the incision was extended and the peritoneum opened to allow safer dissection (Figure 3A, 3B). The cyst was completely resected without rupture. A portion adherent to the bladder dome was excised en bloc, necessitating a partial cystectomy (Figure 3C), followed by single-layer bladder closure and a negative leak test. Two Redon drains and a Foley catheter were placed postoperatively.
_supravesical_hydatid_cyst_(yellow_arrow)_adherent_to_the_periton.png)
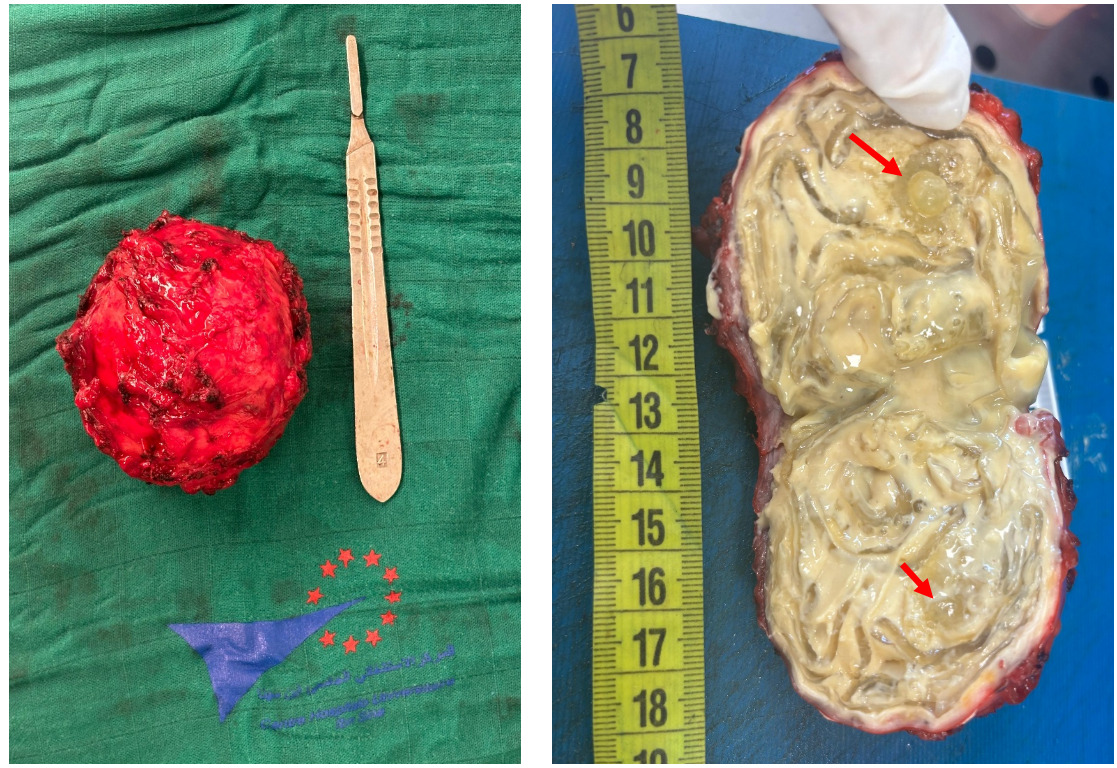
Gross examination of the surgical specimen confirmed the diagnosis of hydatid disease, revealing daughter vesicles (Figure 4).
.png)
The postoperative course was uneventful. The patient was started on albendazole therapy, and regular follow-up was planned.
Discussion
Our case of a supravesical hydatid cyst illustrates an uncommon extrahepatic manifestation of echinococcosis, presenting without typical risk factors or exposure history, and underscores the diagnostic challenges posed by atypical localizations.
Echinococcosis is a zoonotic infection caused by the larval stage of Echinococcus spp., leading to cystic lesions that primarily affect the liver and lungs.4,5 Humans are accidental intermediate hosts, infected through ingestion of parasite eggs from domestic or wild canids. While hepatic and pulmonary sites are most common, extrahepatic localizations are rare, with pelvic hydatid cysts being particularly uncommon.2,3
The disease progresses slowly and is often asymptomatic, with symptoms arising from mass effect or complications such as rupture, secondary infection, or anaphylaxis .4,5 Extrahepatic cysts may be misleading and pose diagnostic challenges, especially in patients without known risk factors or suggestive epidemiological history.
Diagnosis relies on imaging and serology. Serologic sensitivity is moderate in extrahepatic forms (30–70%), while eosinophilia may be present in one-third of cases.6 Ultrasound is the first-line imaging modality, useful for classification (Gharbi, WHO-IWGE), while CT and MRI provide better anatomical detail and assess complications .7,8 Contrast-enhanced ultrasound (CEUS) may help evaluate cyst viability.9
Albendazole (10–15 mg/kg/day) is the cornerstone of medical therapy, used alone in selected cases or as perioperative treatment. It is contraindicated in large, calcified cysts, severe liver disease, and during early pregnancy. Response rates vary: 10–30% cure, 50–70% clinical improvement, and 20–30% non-response.2,5,6,9
Surgical treatment is reserved for large cysts, symptomatic lesions, or those at risk of rupture or causing compression of adjacent structures. The choice of technique depends on the cyst’s location, accessibility, and degree of adhesion. In some cases, partial resection or bladder-sparing procedures may be necessary. Perioperative albendazole is recommended to minimize the risk of recurrence or secondary hydatidosis .2,5,6,9
PAIR (puncture, aspiration, injection, reaspiration) is a minimally invasive option for selected hepatic or abdominal cysts, but is contraindicated in pulmonary locations. MoCAT (Modified Catheterization Technique), combining aspiration, membrane removal, and catheter drainage, is suitable for non-complicated CE2 and CE3b cysts .3,4,6
For inactive cysts (CE4/CE5), WHO-IWGE recommends a watch-and-wait approach in asymptomatic patients.2,3
This case aligns with previous reports of atypical hydatid disease2,3 and further illustrates the potential for isolated pelvic presentations to mimic other benign or malignant masses, thereby reinforcing the critical role of imaging, serology, and intraoperative findings in guiding diagnosis and treatment.
Conclusion
This case highlights an exceptional supravesical pelvic localization of hydatid disease in a patient without apparent risk factors. It underscores the need to maintain a high index of suspicion for any pelvic mass of uncertain origin, even in non-endemic urban settings. Individualized surgical intervention, combined with antiparasitic therapy and close follow-up, remains essential to ensure optimal outcomes and prevent recurrence.
Ethics approval and consent to participate
Ethical approval is not applicable. The case report is not containing any personal information.
Consent for publication
Written informed consent was obtained from the patient for publication and any accompanying images.
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
Not applicable
Acknowledgements
Not applicable