INTRODUCTION
Spinal cord transection is not a common condition. This rarity is due to the substantial protection surrounding the spinal cord, which includes layers of skin, subcutaneous fatty tissue, muscles, and the bony framework. However, penetrating spinal cord injuries represent a group of devastating traumas, characterized by the passage of a sharp object through the spinal column, leading to neural or vascular injuries.1 Unfortunately, there is no consensus in literature concerning their management and few articles have treated this question.
We present the case of a 19-year-old patient who suffered a stab wound resulting in a complete transection of the cervical spinal cord.
Spinal cord transection is an uncommon and severe neurological condition, largely attributed to the extensive anatomical protection afforded to the spinal cord. This includes multiple tissue layers such as skin, subcutaneous fat, muscular structures, and most significantly, the vertebral column. Nonetheless, penetrating spinal cord injuries (PSCIs) constitute a rare subset of spinal trauma, typically resulting from the traversal of a sharp object through the spinal canal. These injuries frequently cause profound neurological deficits due to direct mechanical disruption of neural or vascular elements.1
The clinical and radiological evaluation of such injuries is essential to determine the extent of neural damage and to guide therapeutic decisions. Magnetic Resonance Imaging (MRI) remains the modality of choice for evaluating spinal cord integrity, allowing for detailed visualization of transection, edema, hemorrhage, or cord compression. Computed Tomography (CT), on the other hand, provides superior assessment of bony structures and foreign body trajectories, and is often the first-line imaging tool in acute settings.2,3
Despite the potential for catastrophic outcomes, there is currently no standardized management protocol for PSCIs, particularly in cases of complete cord transection. Literature on this topic remains sparse, with most reports limited to case studies or small series. Here, we describe the case of a 19-year-old male who sustained a cervical spinal cord transection following a stab wound, aiming to highlight the clinical presentation, radiological findings, and considerations for management.
CASE REPORT
A 19-year-old patient with no medical history was admitted to the emergency department with a knife stab wound to the posterior and middle cervical region following an assault. Clinical examination revealed several superficial stab wounds on the face and upper back, with a deeper wound in the posterior neck area. There was no apparent bleeding or cerebrospinal fluid leak. No foreign body was present, suggesting that the knife was removed during the altercation. He denied loss of consciousness or shortness of breath. He was alert and oriented, with a neurological examination revealing a complete loss of sensory and motor function below the neck, consistent with C4 dermatomal levels, explaining the quadriplegia and sphincter dysfunction (ASIA A). Hemodynamic and respiratory functions were stable, and there were no associated injuries.
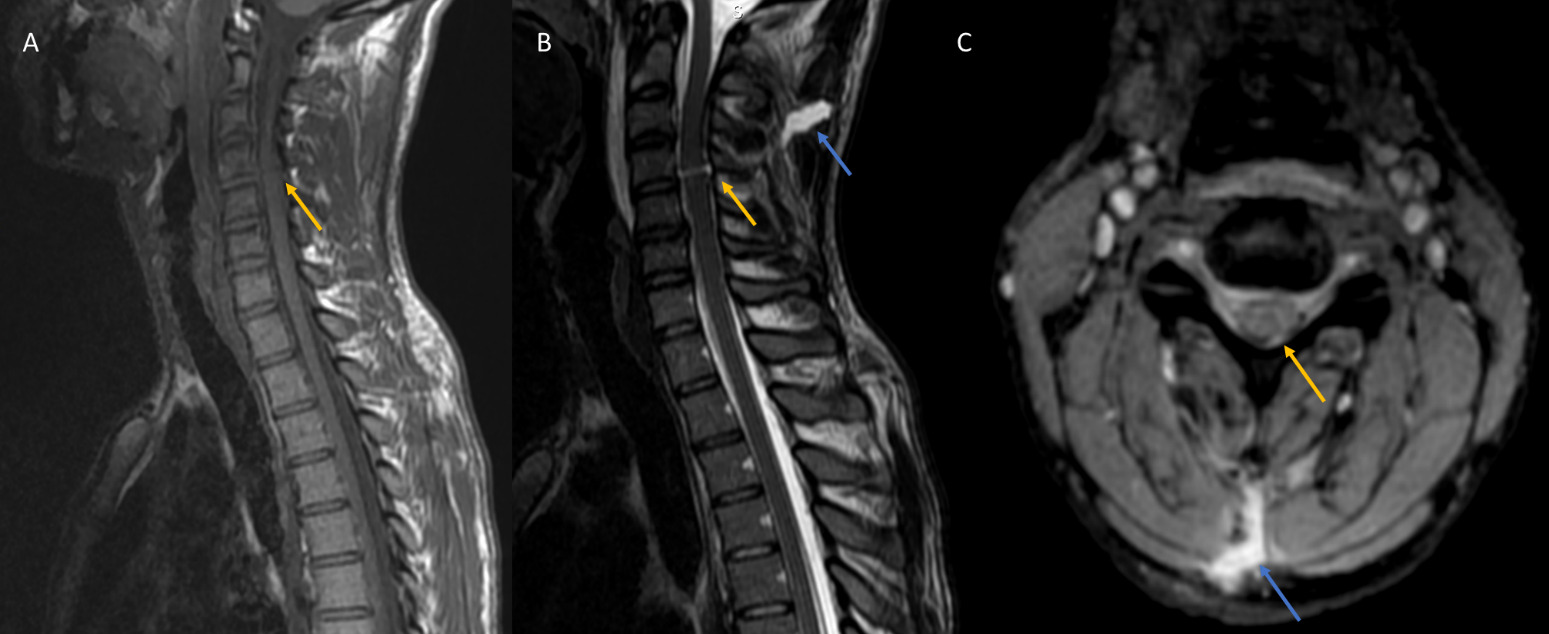
A spine MRI was performed, showing a disruption of the interspinous ligaments between C4 and C5, with a linear band in the spinal cord, hypointense signal on T1 and hyperintense signal on T2, corresponding to a complete transection of the cervical spinal cord at the level of C4, explaining the quadriplegia and the absence of breathing abnormalities. The continuity of the T2 hyperintense signal in the midline soft tissue corresponds to the knife tract (Figure 1).
__sagittal_(b)_and_axial_t2-weighted_(c)_images_sh.png)
The patient was admitted to the ICU, and since there was no foreign material to remove, nor hemorrhage or collection to drain, he did not undergo surgical treatment. Instead, a conservative approach was preferred, based on painkillers, empirical antibiotics, and physical therapy. He remained neurologically stable, but unfortunately, he died 4 days later from severe pneumonia.
DISCUSSION
Penetrating spinal cord injuries are rare, representing 5,5% of spinal cord injuries.2 They are usually inflicted with knives and generally have a low incidence rate, with a challenging clinical long-term follow-up.3 This explain the lack of consensus in literature on how to manage it.
The mechanism of neurological disability can be explained either by a primary lesion of the vascular or neurological structures, or secondary to compression with edema and inflammation in the spinal cord.2
Depending on the affected area, clinical examination can reveal minimal neurological loss, sensitive/sensorial deficiency or Brown Sequard syndrome to complete quadriplegia with sphincterial disorder. This could be assessed with the American Spinal Injury Association Impairment Scale (ASIA).
Management of penetrating spinal cord injury remains controversial with no consensus.4 The diagnosis is confirmed through radiological examination such as plain X-ray, CT scan or MRI, to determine the level and type of spinal injury, but also to detect hematoma or retained foreign body.2
Initially, imaging modalities should be performed depending on the presence or absence of the penetrating agent. In this case, a plain X-ray or, preferably, a CT-scan is indicated to determine the knife tract and location so it can be safely removed. MRI is not routine and should be reserved—after stabilization and projectile safety assessment—for unexplained neurological deficits or suspected ligaments and spinal cord injury, including contusions, hematoma and extramedullary compression Vascular assessment with contrast-enhanced sequences is also warranted to identify repairable lesions.5 Our patient performed an MRI at his admission, revealing a complete transection of the cervical cord and a knife-tract damage, with no sign of hematoma or dural compression.
The conservative or surgical approach for these patients also remains a subject of controversy.4 If there is a need for foreign body removal, wound debridement, spinal decompression, persistent symptomatic cerebrospinal fluid leak repair, or stabilization procedures, surgical treatment is required.1 Our patient didn’t have none of this, so a conservative approach was preferred.
On the other hand, conservative modalities are used in non-surgical cases and consist of empiric antibiotics, steroids to reduce edema, and physical therapy, which increases the chance of spontaneous recovery.2,6
The use of antibiotics is necessary to prevent infections, while the use of corticosteroids remains controversial. Indeed, while some studies have concluded that there is a benefit to their use within the first 8 hours after the incident, other studies have shown no difference between the group receiving corticosteroids and the group that does not.4
Despite common assumptions, the prognosis for these patients is not uniformly poor, as several documented cases have demonstrated significant improvement and recovery of neurological function.2,5
CONCLUSION
Penetrating knife injuries to the spinal cord are relatively rare, and few case reports exist in the literature. Direct stab injuries to the spinal cord are rarely encountered. Whereas incomplete spinal cord injury is common, complete transection of the spinal cord remains very rare, and the treatment can either be surgical or conservative, depending on the associated lesion. Due to the limited data, further investigations are needed to establish best management strategies.
PATIENT CONSENT
Written informed consent for publication was obtained from the legally authorized representative of the patient.