

Introduction
Rotator cuff injuries are among the most common causes of shoulder pain in athletes; however, isolated subscapularis (SSC) tendon tears are distinctly uncommon, accounting for less than 4.9% of all rotator cuff injuries.1 Subscapularis function is essential for internal rotation, anterior stability, and dynamic control of the glenohumeral joint, particularly in overhead athletes such as swimmers.2 While supraspinatus and infraspinatus tears are frequently reported, Under-recognition of subscapularis tears is partly attributable to the limited sensitivity of ultrasound, which detects only about 40% of cases and performs especially poorly in smaller type I–II tears.3
Isolated intrasubstance SSC tears present additional diagnostic challenges, as clinical signs such as lift-off and belly-press may be absent or inconclusive.4 Standard Magnetic Resonance Imaging (MRI) and ultrasound can miss these subtle lesions, although radial-slice MRI sequences have improved sensitivity.5 Arthroscopy therefore remains the gold standard for both diagnosis and definitive management.6
The management strategies of SSC tears have evolved considerably, with arthroscopic repair demonstrating superior outcomes to open techniques, particularly in athletes requiring rapid and safe return to play.7 Here, we present a rare case of an isolated intrasubstance SSC tear in a competitive swimmer, successfully managed with arthroscopic transtendinous repair and structured rehabilitation, achieving excellent clinical and functional results and highlighting the importance of early recognition, accurate diagnosis, and tailored surgical intervention.
Case Presentation
A 21-year-old elite competitive male swimmer admitted through orthopedics / Sports Medicine with an eight-month history of progressive right anterior shoulder pain. The pain worsened with internal rotation during strokes, particularly the freestyle and butterfly techniques. The athlete reported associated weakness during resisted internal rotation and difficulty maintaining training intensity, but no history of acute trauma. Conservative measures including rest, physiotherapy, and NSAIDs provided minimal relief.
The patient had no significant past medical or surgical history and presented with stable vital signs: blood pressure ~ 120/75 mmHg, body temperature ~36.8°C, respiratory rate ~16/min, heart rate ~ 72 bpm. Although his heart rate was slightly higher than the bradycardia baseline often observed in trained athletes, it was still within the physiological normal range.
On clinical examination, there was tenderness localized to the anterior shoulder. The belly-press and lift-off tests elicited pain but only mild weakness. External rotation strength and supraspinatus testing were normal. No evidence of instability or generalized ligamentous laxity was observed. A comprehensive differential diagnosis includes: supraspinatus tear, infraspinatus tear, biceps pulley lesion, subacromial impingement, labral tear, and shoulder instability.
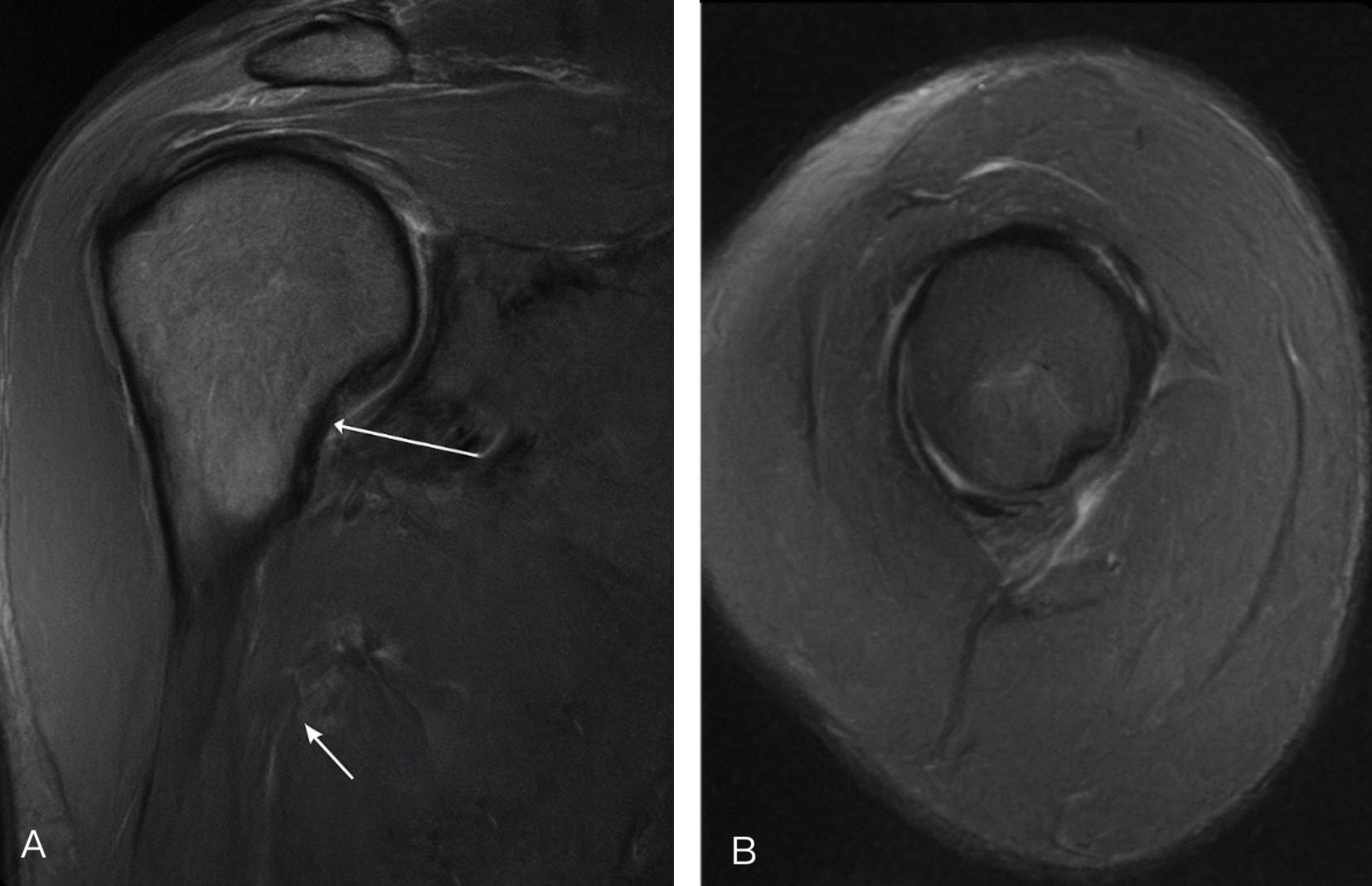
Magnetic resonance imaging (MRI) revealed an intrasubstance tear of the upper one-third of the subscapularis tendon consistent with a Lafosse IIA lesion (Figure 1). The tear was confined to the tendon substance without detachment from the lesser tuberosity. The supraspinatus, infraspinatus, and teres minor tendons were intact, and no associated biceps pulley injury was observed.
Diagnostic arthroscopy confirmed a well-defined intrasubstance split in the upper subscapularis fibers with fraying but preserved lateral insertion (Figure 2). The lesion was repaired transtendinously using a knotless all-suture anchor system, allowing preservation of intact lateral fibers. Stability was restored following fixation, with no iatrogenic injury to adjacent structures.

The patient was immobilized in a sling for four weeks, with early initiation of passive range of motion exercises. At six weeks, active-assisted and progressive strengthening exercises were introduced, focusing on internal rotation endurance and dynamic stability. Sport-specific rehabilitation, including swimming stroke simulations and resistance band drills, commenced at 12 weeks.
By six months, the patient had returned to competitive swimming without pain or restriction. At 12-month follow-up, clinical examination revealed full shoulder range of motion, 5/5 strength in internal rotation, and no tenderness (Table 1). Functional outcome scores demonstrated excellent results, with a Constant score of 94 and an American Shoulder and Elbow Surgeons (ASES) score of 98.
Discussion
Isolated intrasubstance subscapularis (SSC) tears are rarely reported in the literature. Most SSC lesions occur in conjunction with supraspinatus or biceps pulley pathology, which makes this presentation unusual.8 Lafosse et al. classified subscapularis tears into five types, with type II lesions representing partial tears confined to the upper portion.9 Intrasubstance variants, as in this case, are particularly elusive, as clinical tests such as the lift-off or belly-press may be equivocal.5
Although MRI is widely accepted as the gold standard for rotator cuff imaging, its sensitivity for detecting subscapularis tears has been reported to be as low as 37–40% in some studies.6 High-resolution sequences and arthroscopic confirmation are often required. Prior reports suggest that untreated subscapularis lesions may progress, leading to pain, dysfunction, and further tendon degeneration.10
Arthroscopic management has evolved as the preferred approach, offering enhanced visualization and minimally invasive repair. Several studies report favourable outcomes with arthroscopic repair of partial subscapularis tears, particularly in athletes.11 However, few cases describe successful return to high-level overhead sports following intrasubstance repair. The use of knotless all-suture anchors in this case provided stable fixation while preserving intact fibers, minimizing the risk of overtensioning or tissue damage.
Rehabilitation remains critical, particularly in athletes. Literature emphasizes phased mobilization, gradual strengthening, and tailored sport-specific progression.12 Our patient achieved return to elite-level competition at six months, aligning with timelines reported for supraspinatus repairs but faster than typical recovery from extensive subscapularis reconstructions.13
This report contributes to the scarce evidence on intrasubstance SSC tears in swimmers. Its strengths lie in the comprehensive diagnostic evaluation with MRI, arthroscopic confirmation, and relatively long-term follow-up with validated outcome measures. However, the report is limited by its single-patient design and lack of direct comparative data. Further studies are required to better define the prognosis and optimal management strategies in this subset of athletes.
Conclusion
Isolated intrasubstance subscapularis tears are uncommon but can have a substantial impact on shoulder function in competitive swimmers. Accurate diagnosis requires high-resolution imaging and careful arthroscopic evaluation, as these tears may be missed on routine clinical assessment. Arthroscopic transtendinous repair using knotless anchors, combined with a structured, phase-wise rehabilitation protocol, resulted in full recovery of range of motion, strength, and return to competitive swimming within six months. Compared with previous reports, which often describe prolonged recovery or partial functional improvement, this case demonstrates that early diagnosis, meticulous surgical technique, and tailored rehabilitation can achieve excellent functional outcomes and early return to sport. This highlights the need for heightened clinical suspicion of subscapularis pathology in athletes presenting with anterior shoulder pain and reinforces evidence-based strategies for management and rehabilitation.
Ethical Considerations
Written informed consent was obtained from the patient for the publication of this case report and accompanying images. Institutional Review Board (IRB) approval was not required for this single patient case report, in accordance with institutional policies on case reports and non-experimental research.