Introduction
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disorder characterized by insulin resistance and progressive β-cell dysfunction, leading to hyperglycemia and increased risk of microvascular and macrovascular complications.1 Despite advancements in pharmacologic therapies, including metformin, sulfonylureas, GLP-1 receptor agonists, SGLT2 inhibitors, and insulin, many patients remain inadequately controlled, necessitating alternative therapeutic approaches.2 The gastrointestinal tract, especially the duodenum, is central to nutrient sensing and regulates the release of incretin hormones such as GLP-1 and GIP, which promote insulin secretion and enhance insulin sensitivity.3 In individuals with T2DM, this enteroendocrine function is often impaired, contributing to dysregulated glucose homeostasis.3
Duodenal mucosal resurfacing (DMR) represents a new endoscopic intervention that seeks to re-establish healthy duodenal architecture and physiological function.4 It employs hydrothermal ablation of the mucosal surface, which promotes regeneration and may recondition enteroendocrine activity.4 Early clinical studies have demonstrated its feasibility, safety and efficacy in improving glycemic control in patients with T2DM,5 mimicking some of the metabolic effects of bariatric surgery without the associated risks and invasiveness.6 Notably, a multicenter, open-label study reported significant reductions in HbA1c and insulin requirements up to 12 months post-procedure, with minimal adverse events.7 These findings suggest that DMR may offer a promising adjunctive treatment for patients with refractory T2DM. We present this case to illustrate the use of DMR in a patient with long-standing refractory T2DM who achieved rapid and significant reduction in HbA1c and insulin requirements without complications.
Case Presentation
A 54-year-old male with a 12-year history of type 2 diabetes mellitus (T2DM) who was referred for further evaluation owing to persistently elevated glucose levels despite adherence to oral therapy (metformin 1000 mg twice daily, glimepiride 4 mg daily) and basal–bolus insulin totaling 80 units daily. The patient also has a history of hypertension, controlled with amlodipine, and dyslipidemia managed with atorvastatin. There was no history of diabetic complications, including neuropathy, retinopathy, or nephropathy. Family history was positive for T2DM in first-degree relatives.
On presentation, the patient’s vital signs were within normal limits: temperature 36.8°C, blood pressure 128/82 mmHg, respiratory rate 16 breaths per minute, heart rate 84 beats per minute, and oxygen saturation 98% on room air. The physical exam revealed central obesity, with a body mass index of 31 kg/m² and a waist circumference of 105 cm. Mild acanthosis nigricans was noted on the neck and axillae. Laboratory evaluation revealed an HbA1c of 10.2% and an average fasting glucose of 220 mg/dL over the prior three months. Lipid profile showed elevated triglycerides (220 mg/dL), and liver and renal function tests were within normal limits (Table 1). The patient reported adherence to a balanced diet and engagement in moderate physical activity.
The patient underwent duodenal mucosal resurfacing (DMR) with the Revita system (Fractyl Laboratories, Waltham, MA, USA) under conscious sedation. A catheter was inserted into the duodenal bulb, and circumferential hydrothermal ablation was performed on a 9 cm segment of the post-pyloric duodenum, with each segment treated at 90°C for 10 seconds.
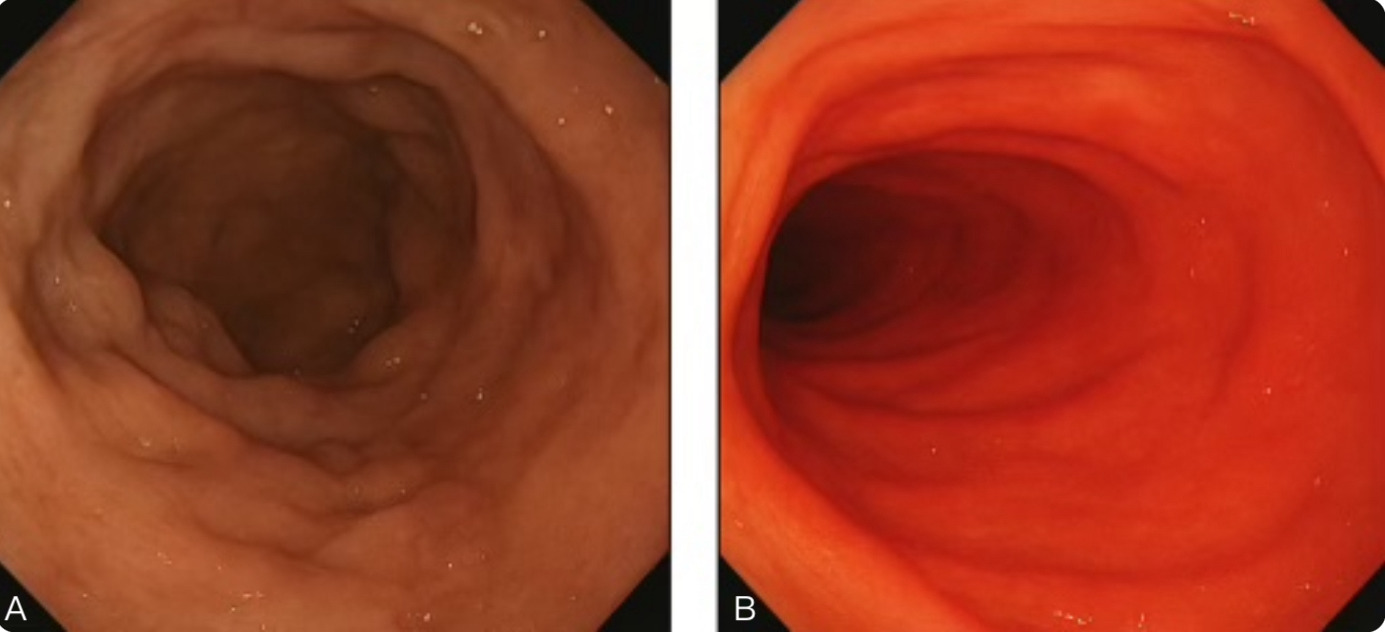
Endoscopic images during the procedure revealed that the duodenal mucosa appeared normal preceding the hydrothermal ablation, but with subtle irregularities consistent with T2DM-related mucosal changes. Following circumferential hydrothermal ablation, the treated segment showed a uniform, erythematous appearance, indicating successful mucosal resurfacing (Figure 1). These images visually confirm the extent and completeness of the DMR procedure.

The total procedure time was approximately 45 minutes, and no intra-procedural complications occurred. The patient was monitored overnight and discharged the following day. Post-procedure follow-up was conducted at 1, 2, and 3 months, with the HbA1c decreasing progressively to 8.2% at 1 month, 7.6% at 2 months, and 7.1% at 3 months. Fasting glucose was normalized to 110 mg/dL, and total daily insulin requirements were reduced by 50% (Table 2). The patient reported increased energy, improved mood, and better overall quality of life, and notably no adverse events, including nausea, abdominal pain, or gastrointestinal bleeding.
This case demonstrates that DMR can lead to rapid and significant improvements in glycemic control and insulin requirements in patients with refractory T2DM. No peri-procedural or delayed complications were observed. The patient was clinically stable during the procedure, tolerated the intervention without adverse effects, and reported no pain, nausea, or gastrointestinal symptoms during the 3-month follow-up period, thereby demonstrating the excellent safety and tolerability of DMR in this case, supporting its role as a promising adjunctive therapy.
Discussion
Type 2 diabetes mellitus (T2DM) is a progressive metabolic disorder, and a subset of patients remain poorly controlled despite intensive treatment with multiple oral antidiabetic agents and high-dose insulin.8 This report underscores the potential of DMR as an emerging endoscopic therapy for patients with poorly controlled type 2 diabetes. Our patient had long-standing disease with suboptimal glycemic control despite maximal medical therapy, yet experienced marked improvement following DMR.
The duodenum plays a central role in glucose homeostasis through nutrient-stimulated secretion of incretin hormones, including glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), which enhance insulin secretion and sensitivity.8 DMR targets the diseased duodenal mucosa by hydrothermal ablation, leading to mucosal regeneration, normalization of enteroendocrine signaling, and improved glycemic control.9 The procedure resulted in clinically relevant improvements, including lower HbA1c, reduced insulin dependence, and positive changes in the patient’s energy, mood, and daily functioning.
These findings are consistent with published data. Clinical trials have demonstrated durable HbA1c reductions and decreased insulin use lasting up to 12 months after DMR.10 In one multicenter trial, mean HbA1c decreased by 1.3% at six months, closely mirroring the improvement observed in our patient.11 Importantly, DMR has a favorable safety profile, with most adverse effects being mild and transient and serious complications occurring rarely.12 This makes DMR an attractive option, particularly for patients who are not candidates for bariatric surgery or prefer a minimally invasive solution.13
Nevertheless, important limitations remain. Long-term data on the durability of glycemic benefit and impact on diabetes-related complications are still limited. Ongoing trials are evaluating its effects on cardiovascular outcomes, kidney function, and patient-reported quality of life.14,15
This case report also has specific strengths, including comprehensive baseline and follow-up data (clinical, biochemical, and anthropometric), serial HbA1c and fasting glucose measurements, and detailed procedural documentation with endoscopic images confirming technical success. Patient-reported improvements in energy and mood add valuable insight into quality-of-life changes.
However, several limitations must be acknowledged. Given that this is a single-patient case, the findings are not generalizable, and variability in how patients respond to DMR may be substantial. The three-month follow-up period further restricts the ability to assess lasting efficacy and safety. Furthermore, the lack of a standardized quality-of-life instrument and comparator arm precludes robust comparison with established treatments.
Overall, this case underscores DMR’s promise as a safe and effective adjunctive therapy for refractory T2DM when conventional therapies fail. While early outcomes are encouraging, further large-scale, long-term studies are needed to confirm its durability, safety, and potential role in standard diabetes care.
Conclusion
Duodenal Mucosal Resurfacing (DMR) is an emerging endoscopic technique that targets the duodenum’s involvement in glucose metabolism, offering a new therapeutic approach for patients with refractory type 2 diabetes. In our case, DMR led to rapid and substantial improvements in glycemic control and reduced insulin requirements, highlighting its potential as an effective adjunctive therapy for patients inadequately controlled with conventional treatments.
While current evidence and growing clinical experience suggest that DMR is safe and efficacious, long-term outcomes, patient selection criteria, and the durability of its metabolic effects require further investigation. This case adds to the emerging body of literature supporting DMR as a promising non-surgical therapeutic option and underscores the need for continued research to define its role in future diabetes care.
Ethical Considerations
Written informed consent was secured from the patient for publishing the case details and images. IRB approval was not required for this non-experimental, single-patient report.