Introduction
Stenotrophomonas maltophilia is an aerobic Gram-negative, non-fermentative bacillus that was first isolated in 1943 as Bacterium bookeri, later renamed multiple times due to genetic and phenotypic analyses.1 S. maltophilia is the third most frequent nosocomial pathogen among non-fermentative bacteria, following Pseudomonas aeruginosa and Acinetobacter spp.2 S. maltophilia is an environmental organism that can be isolated from various sources in nature, including water, soil, plants, and animals. It has also been isolated from human faeces, frozen fish, woodland ticks, and raw milk, and also can be transmitted by nosocomial sources, including intravenous fluids, catheters, central venous and dialysis equipment, ventilation circuits. Due to its intrinsic resistance to broad-spectrum antibiotics, including β-lactams and carbapenems, it becomes increasingly recognized as a cause of nosocomial infections.3,4 While it typically affects immunocompromised patients, such as those with prolonged hospital stays, broad-spectrum antibiotic usage, hematologic malignancies, indwelling medical devices, HIV patients, or chronic pulmonary diseases like cystic fibrosis, its occurrence in immunocompetent individuals, particularly following routine surgical procedures, remains exceedingly rare.5–7 Reported mortality rates range from 18% to 69%, largely due to diagnostic delays and the limited availability of effective treatment options.8 Despite its clinical significance, S. maltophilia remains understudied, posing ongoing challenges in early identification and targeted therapy.
Case Presentation
A 38-year-old previously healthy male with no significant past medical history and no family history of immunodeficiency or relevant hereditary conditions. The patient underwent elective knee arthroscopy for a meniscal tear. The procedure was uneventful, and the patient was discharged the same day with routine postoperative care instructions and no antimicrobial prophylaxis beyond standard perioperative dosing.
On postoperative day seven, the patient developed a high-grade fever (up to 39.5°C), chills, malaise, and localized discomfort in the operated knee, accompanied by mild swelling. He returned to the emergency department with stable vital signs, except for tachycardia (110 bpm) and low-grade hypotension (blood pressure 95/60 mmHg). Physical examination revealed erythema and tenderness around the surgical site without signs of wound dehiscence or purulent discharge. Laboratory investigations demonstrated leucocytosis (white blood cell count: 14,800/μL), a markedly elevated C-reactive protein level (180 mg/L), and a raised procalcitonin level (4.5 ng/mL), raising concern for postoperative infection and early sepsis (Table 1).
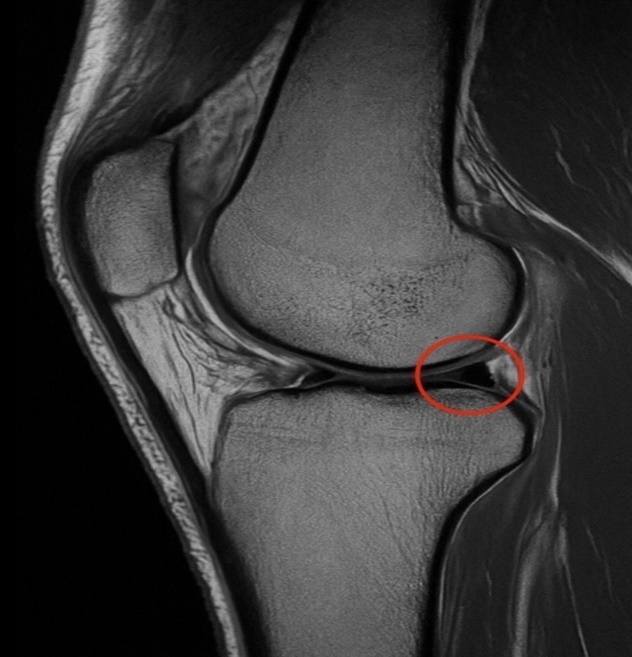
Empiric broad-spectrum intravenous antibiotics were initiated with meropenem and vancomycin, and two sets of blood cultures were drawn. Imaging with MRI of the knee ruled out joint effusion or deep abscess formation (Figure 1).

T2-weighted sagittal MRI of the right knee revealing a horizontal tear in the posterior horn of the medial meniscus
Within 48 hours, blood cultures yielded growth of Stenotrophomonas maltophilia in both sets. Antibiotic susceptibility testing revealed resistance to beta-lactams (98%), carbapenems (100%), and aminoglycosides (95%), while maintaining susceptibility to trimethoprim-sulfamethoxazole (85%) and minocycline (90%) (Table 2).
Diagnostic challenges included septic arthritis and surgical site infection (SSI) due to Staphylococcus aureus, the most common postoperative infections. The patient’s lack of response to empiric antibiotics and an unusual resistance profile delayed targeted therapy, highlighting the importance of culture-driven management in atypical postoperative infections. The initial challenge was the uncommon identification of S. maltophilia, a multidrug-resistant pathogen that posed both a diagnostic and therapeutic challenge. Empiric therapy with meropenem and vancomycin had no coverage for S. maltophilia.
Given the intrinsic resistance profile of Stenotrophomonas maltophilia, empiric antibiotics were discontinued and replaced with intravenous trimethoprim-sulfamethoxazole (15 mg/kg/day based on the trimethoprim component, in divided doses) and oral minocycline (100 mg twice daily). Antibiotics were well tolerated with no reported side effects or allergic reactions. The patient showed rapid clinical improvement within 72 hours, with defervescence, normalization of inflammatory markers, and negative follow-up blood cultures after five days of directed therapy. The patient had initially undergone elective knee arthroscopy, developed symptoms on postoperative day 7, and was diagnosed with multidrug-resistant S. maltophilia bacteraemia on day 9. Targeted therapy led to clinical resolution and negative blood cultures by day 14 (Table 3).
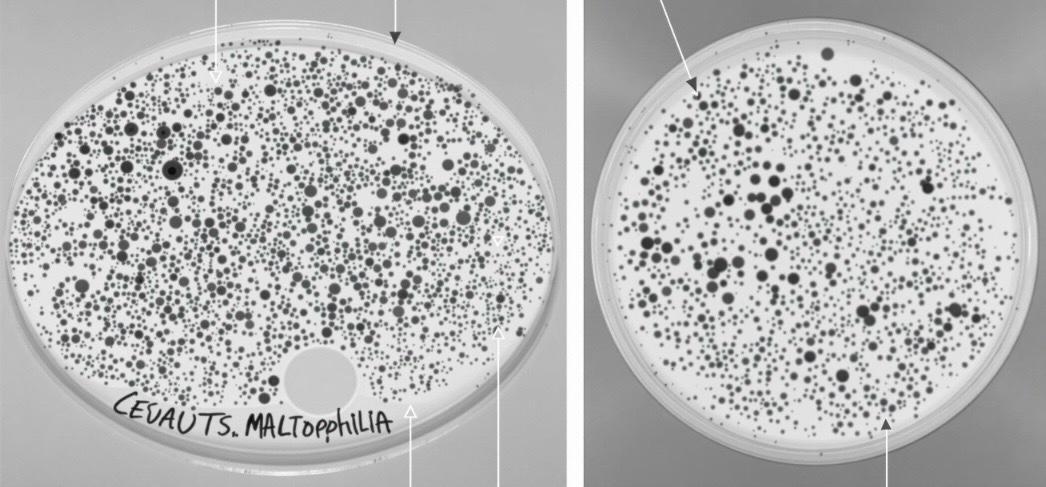
On postoperative day seven, blood cultures were obtained due to persistent febrile episodes and rising inflammatory markers. Within 48 hours, growth was detected in 80% of the blood culture samples on selective media plates. Final identification was confirmed using an automated identification system and selective biochemical assays. The organism exhibited resistance to beta-lactams, carbapenems, and aminoglycosides, while remaining susceptible to trimethoprim-sulfamethoxazole and minocycline findings consistent with known susceptibility patterns of S. maltophilia.9 These results guided the initiation of targeted antimicrobial therapy (Figure 2).

Early microbiological confirmation was critical for timely adjustment of empiric therapy, underscoring the importance of prompt culture evaluation in postoperative infections involving rare, multidrug-resistant pathogens. S. maltophilia may present with systemic features and rapid onset postoperatively, requiring high clinical suspicion for early detection.10 This case highlights the utility of early blood culture analysis and susceptibility-guided therapy to optimize outcomes in rare, multidrug-resistant infections.
Discussion
We present the case of a healthy 38-year-old immunocompetent male who developed bloodstream infection (BSI) due to S. maltophilia following an elective knee arthroscopy. The patient experienced persistent multidrug-resistant S. maltophilia bacteraemia, presenting with fever(39.5°C), leucocytosis (WBC 14,800/μL), and elevated inflammatory markers (CRP 180 mg/L) and localized knee inflammation on postoperative day 7 was initially managed with empiric meropenem/vancomycin with no response.
Blood cultures identified S. maltophilia within 48 hours, revealing resistance to β-lactams, carbapenems, and aminoglycosides while susceptibility to trimethoprim-sulfamethoxazole (TMP-SMX) and minocycline. An environmental investigation was conducted, as S. maltophilia is often linked to hospital water sources and equipment, suggesting a likely nosocomial origin despite standard precautions. No formal infection control measures were implemented, as this was an isolated case; however, similar future occurrences may warrant internal review to identify potential sources and prevent recurrence. Targeted therapy with IV TMP-SMX (15 mg/kg/day) and oral minocycline (100 mg BID) resulted in a reassuringly rapid clinical improvement within 72 hours, including fever resolution, normalization of biomarkers, and negative follow-up cultures by day 14 The rapid recovery in this case highlights the significant benefits of early susceptibility-directed therapy.
Stenotrophomonas maltophilia infections in immunocompetent individuals are uncommon, especially following minor orthopaedic procedures.11 However, rare reports have described infections in similar contexts, including periprosthetic joint infections after hip revision, epidural abscesses post-lumbar discectomy, and soft tissue infections like myositis or cellulitis.12
The favourable outcome in our patient likely resulted from early clinical suspicion, timely microbiological diagnosis, and prompt initiation of susceptibility-guided therapy. Continuous monitoring with laboratory markers and follow-up cultures further supported the treatment response. Nonetheless, limitations include the absence of surgical site biopsy and the inherent lack of generalizability in a single case report.
Therapeutically, S. maltophilia poses significant challenges due to intrinsic resistance mechanisms.13 These include chromosomally encoded β-lactamases L1 and L2, regulated by the AmpR system, as well as rising resistance to TMP-SMX mediated by mobile genetic elements (e.g., sul1, dfrA).14 Efflux pumps like SmeYZ and virulence factors such as biofilm formation, quorum sensing, and outer membrane vesicles (OMVs) further enhance pathogenicity and antibiotic evasion.15 This case reinforces the importance of considering S. maltophilia in atypical postoperative infections, even in healthy patients, and highlights the effectiveness of early, targeted antimicrobial therapy in achieving successful outcomes.
Conclusion
Stenotrophomonas maltophilia is an emerging multidrug-resistant pathogen that can complicate even minor surgeries in immunocompetent patients. This case emphasizes the importance of considering atypical organisms when postoperative infections do not respond to standard antibiotics. Early culture-based diagnosis and targeted therapy were key to recovery.
The infection despite standard prophylaxis raises the need for heightened clinical awareness and possible reassessment of prophylactic strategies in high-risk settings, guided by local resistance patterns.
Ethical Considerations
Written informed consent was obtained from the patient for the publication of this case report.