
Case Presentation
A 20-year-old male with complete immunizations and no significant medical history, aside from previous Epstein-Barr virus (EBV) infection, presented with acute unilateral facial swelling following two days of flu-like symptoms (rhinorrhea, malaise and fever of 38.5° C). Examination showed a firm, tender, non-fluctuant swelling over the right parotid gland (figure 1).
.png)
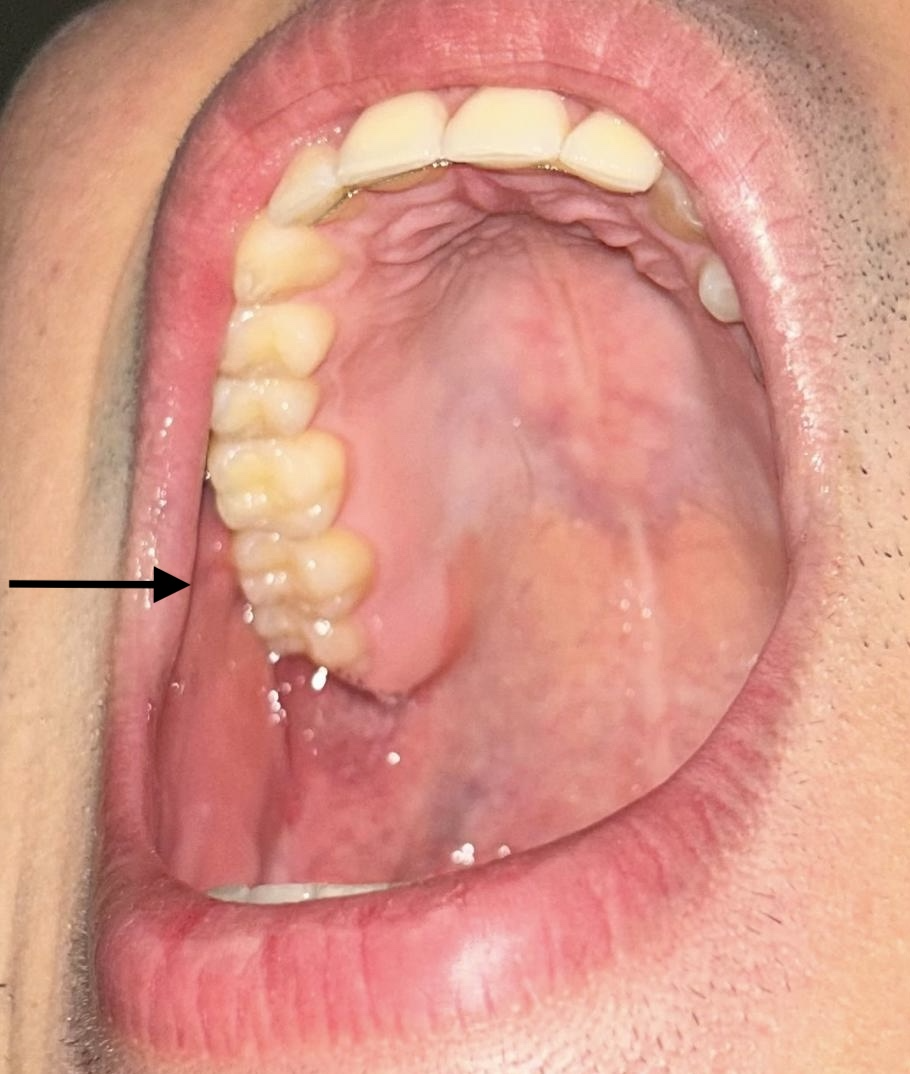
Pain worsened with mastication. Intraoral examination revealed a normal Stensen’s duct without sialolithiasis or purulent discharge (Figure 2). Saliva drainage was normal, with no oral lesions, dental decay, or lymphadenopathy.

Testicular examination and dental radiography were unremarkable. A nasopharyngeal swap tested positive for influenza A (H3N2), negative for influenza B and SARS-CoV-2. Given the patient’s vaccination status and no local mumps outbreak, mumps was unlikely. Human immunodeficiency virus (HIV) was excluded by history; EBV reinfection was improbable. Additional viral etiologies (CMV, Coxsackie A, parainfluenza) were not serologically tested, due to the mild, self-limiting course. Bacterial parotitis was unlikely in the absence of purulence or risk factors. Autoimmune and drug-induced causes were excluded by clinical context. A diagnosis of exclusion was made, with influenza A considered most likely. Treatment with oseltamivir, hydration, and analgesia led to complete resolution within 48 hours.
Diagnosis
Viral non-mumps parotitis secondary to Influenza A
Discussion
Parotitis is classically associated with mumps, with a global incidence of 0.24 per 100,000 individuals.1 In developed nations, vaccination has reduced mumps incidence, while non-mumps etiologies—Coxsackie A virus, CMV, EBV, HIV, parainfluenza, and influenza— are increasingly common.2,3 Less frequent causes include bacterial (Staphylococcus aureus, Mycobacterium tuberculosis), autoimmune (Sjögren’s, rheumatoid arthritis, lupus), and drug-induced parotitis.4 Influenza-associated parotitis is rare but increasingly recognized. During the 2014–2015 influenza season, the CDC reported over 300 cases, primarily H3N2 related.2 It occurs more often in males and school-aged individuals.2
Differentiating mumps from non-mumps parotitis is essential due to differing clinical courses. Mumps usually causes bilateral swelling and systemic symptoms; viral non-mumps parotitis tends to be unilateral, acute, brief and less likely to cause complications.5 Diagnostic testing—serologies, inflammatory markers, mumps titers, imaging, and cultures—can clarify etiology.4
Accurate diagnosis also has public health implications.2,6 Misdiagnosing influenza as mumps may lead to unnecessary isolation, inaccurate surveillance, and missed antiviral therapy.3 Failure to identify mumps in under-vaccinated populations may fuel outbreaks.2 Timely recognition also prevents inappropriate antibiotics and diagnostic overuse.
Although rarely considered, influenza should remain on the differential of parotitis, especially during flu season or when mumps incidence is low, as greater awareness ensures appropriate diagnosis, treatment, and public health response.6