
Introduction
Ischemic pontine strokes are a form of stroke caused by a blockage either in the pontine or vertebrobasilar arteries. These blockages result in infarcts in the pons portion of the brainstem. Located between the midbrain and medulla, the pons is responsible for movement, sensory function, balance, heartbeat, and a myriad of other crucial functions. This particular stroke occurred in the left half of the pons, meaning that the contralateral (right) side of the body would be most affected by the stroke. Pontine strokes account for 7% of all ischemic strokes.1
There is a stronger incidence correlation for pontine stroke in Black and Hispanic adults; however, there is a lack of epidemiological evidence implying causation in any specific demographic.2 As with many strokes, the risk of a pontine stroke increases as a person grows older. In addition to age, multiple pre-existing conditions can increase the risk of stroke. Common conditions include hypertension, a history of cardiovascular disease, and diabetes. In less common cases, dyslipidemia can also contribute to clotting due to high concentrations of lipids in the bloodstream.3 In rare cases, Pontine Warning Syndrome (PWS), a condition in which blood flow to the pons is limited, exhibits itself as small windows of stroke-like symptoms. PWS is a very strong indication that a pontine stroke will occur in the future.4 Patients with pontine stroke present with symptoms that can include hemiparesis to total hemiplegia, slurred speech, facial drooping, and inhibited mental capacity. In addition to these symptoms, patients frequently complain of nausea, dizziness, or vertigo.2
Case Report
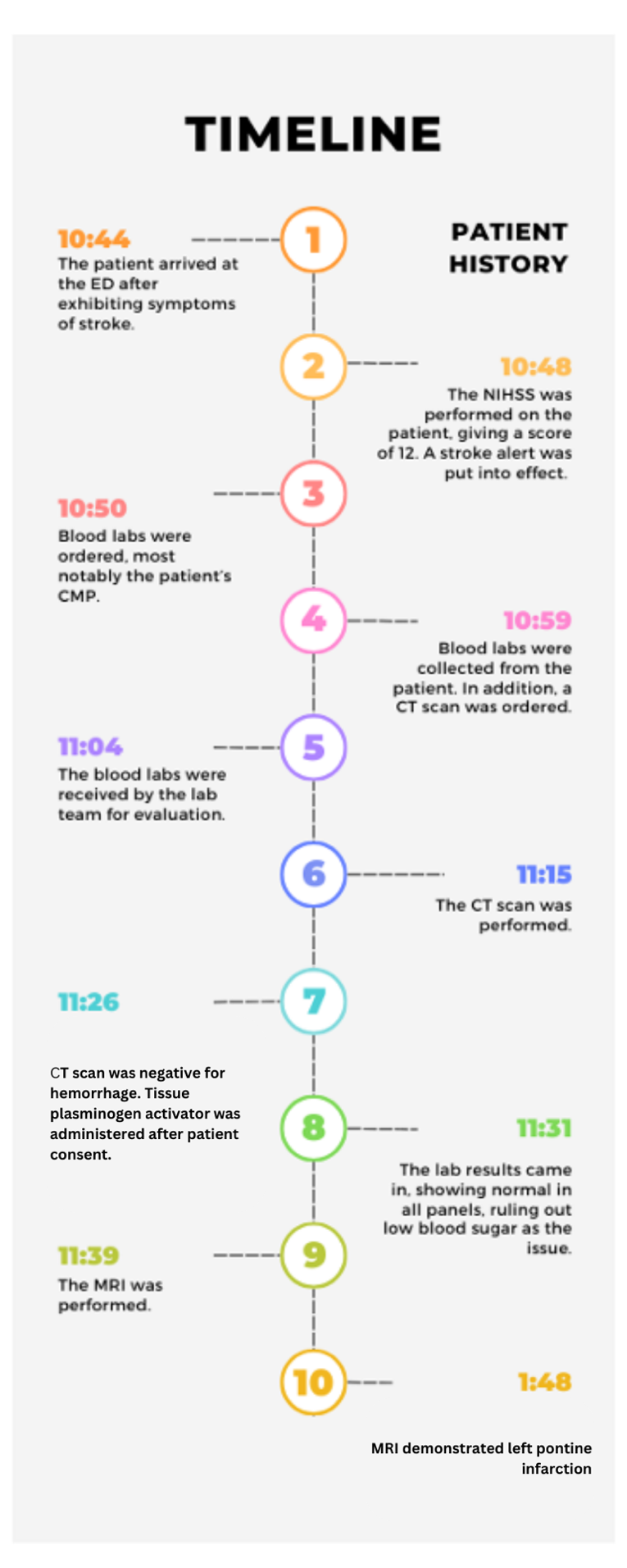
The patient was a 74-year-old African American male with a medical history of hypertension, diabetes, and stroke. The patient’s wife stated that he bent over to pick up an item and could not walk afterward. When he stood back up, he had slurred speech and his “head was swimming.” The patient was given an 81 mg dose of aspirin and was put to sleep in his home by his wife. The patient’s wife also stated that he normally has left-sided weakness due to a previous stroke two years prior. When the patient woke up again, his wife noted right facial droop, dizziness, right side weakness, which was worse than before, and he was taken to the emergency department. His vitals were 98.5° F temperature, 120/100 mm Hg blood pressure, heart rate of 72 beats per minute, and respiratory rate of 20 breaths per minute. His pulse oximetry read 93% on room air. His blood sugar was 140 mg/dL. Brain optimization measures for acute ischemic stroke5 were depolyed. Upon arrival, the National Institute of Health Stroke Scale revealed a score of 12. Laboratory analyses were all normal except for a hemoglobin A1C of 8.0. His electrocardiogram revealed normal sinus rhythm. Noncontrast brain computerized tomography (CT) scan was performed, which was negative for hemorrhage. CT angiogram of the head and neck did not demonstrate a lesion amenable to thrombectomy. He met criteria for thrombolysis, and 0.9 mg/kg alteplase was administered after obtaining informed consent from his wife. Subsequent magnetic resonance imaging (MRI) scan revealed an infarct on the left side of the pons [Figure 1]. The timeline of his emergency department course is summarized in [Figure 2].
_demonstrating_an_infarct_in_the_left_pons_(left_panel)._r.png)

The patient was subsequently admitted to the intensive care unit. On hospital day two, the patient remained intubated and sedated. An echocardiogram revealed diastolic dysfunction and an ejection fraction of 65%. He was extubated on day 3. He underwent speech evaluation and was cleared by speech therapy. The patient was later discharged to inpatient rehabilitation on day 6, where he continued to recover and eventually discharged home to the care of his wife.
Discussion
This patient presented a particular challenge in diagnosis because of the nature of pontine strokes. While typical posterior strokes involve pontine infarcts with simultaneous strokes impacting other regions of the brain, this particular stroke was unique in that the infarction is limited to the pons.2 In addition, it is difficult to see the pons on a CT scan because of the existence of the petrous temporal bone. The artifact blocks the view of the pons and therefore prevents CT scans from detecting these strokes. MRIs, however, allow for clear visualization of the pons and any infarctions that may be present.6 Indeed, MRI has greater sensitivity and specificity in diagnosing acute ischemic stroke compared to CT scan, with ~ 80% of infarcts detected within 24 hours.7
The reason however that MRIs are not used as the routine imaging modality in the ED is because they take longer to perform, and take the patient away from the ED during that time.
In an acute stroke case, time is of the essence, and complications can develop if left undiagnosed. One of the most feared complications that can develop is locked-in syndrome, in which the patient experiences near-complete paralysis short of eye movement.8 Because of the rapid pace of the medical team, the patient did not experience this complication.
Several imaging sequences are used brain MRI. T1-weighted and T2-weighted scans are most common. T1-weighted images are produced by using short repetition time and time to echo, in contrast to T2 images that are employ the opposite.9 In ischemic stroke, T1-weighted MRI shows low signal in the infarcted area after 16-24 hours due to edema, while T2-weighted MRI shows hyperintense signal due to edema at about 8 hours. Thus, T2 images are best early on in stroke, while T1 mages can help visualize the infarct over time. Typically, in an ED stroke setting, the MRI is obtained 8-24 hours after ED arrival, once the patient is hospitalized.
As an African American male, the patient was at increased risk of stroke at baseline, including pontine infraction, supported by his history of hypertension, diabetes, and cardiovascular disease.10 A recent study in the Journal of the National Medical Association that examined various national databases cites hospitalizations for stroke were higher among Blacks compared to Whites, and all-cause, cerebrovascular disease related mortality was highest in non-Hispanic Black or African American individuals. Interestingly, the study also reported that the number of non-Hispanic Black in adult general cardiovascular fellowship programs was disproportionately lower their White counterparts.11 This training disparity was also highlighted in a 2022 article that analyzed the trends in racial and ethnic diversity among vascular neurology fellowships. This study, which covered the years 2006-2018, found that while the percentage of African American trainees remained the same for neurology overall, the percentage for vascular (stroke) neurology showed a marked downtrend.12
Conclusion
Left pontine infarction is a stroke resulting from basilar occlusion. It presents with typical stroke symptoms such as dysarthria, and hemiparesis, and often with dizziness and vertigo as well. MRI can be a crucial adjunct in the accurate diagnosis of pontine stroke. The prognosis of pontine stroke in this case was favorable once it had been identified, and the patient was eventually able to go home. The case is also a reminder of the burden of cerebrovascular disease in our African American community.
Ethical approval
Informed consent was obtained for the publication of this case report. The Orlando College of Osteopathic Medicine’s research committee deemed this work minimal risk and exempt (study #2025-003).