Introduction
Anal fistulas, abnormal connections between the anal canal and perianal skin, frequently arise from infections and abscesses. Managing high trans-sphincteric fistulas is challenging due to the risk of sphincter damage and post-operative incontinence.1–3 Traditional fistulectomy, once the gold standard, can compromise sphincter function.1,4 In contrast, immediate sphincter repair alongside fistulectomy has shown promise, allowing effective fistula excision with reduced incontinence rates.5 Recent studies report healing rates up to 95% with a recurrence rate as low as 3-5%, though outcomes depend on patient factors and surgical expertise.6 Our study assesses this approach in a Sudanese cohort, examining healing, incontinence, and recurrence, especially in comparison to the cutting seton technique, previously noted to yield a low incontinence rate but with chronic pain concerns.3
Methods
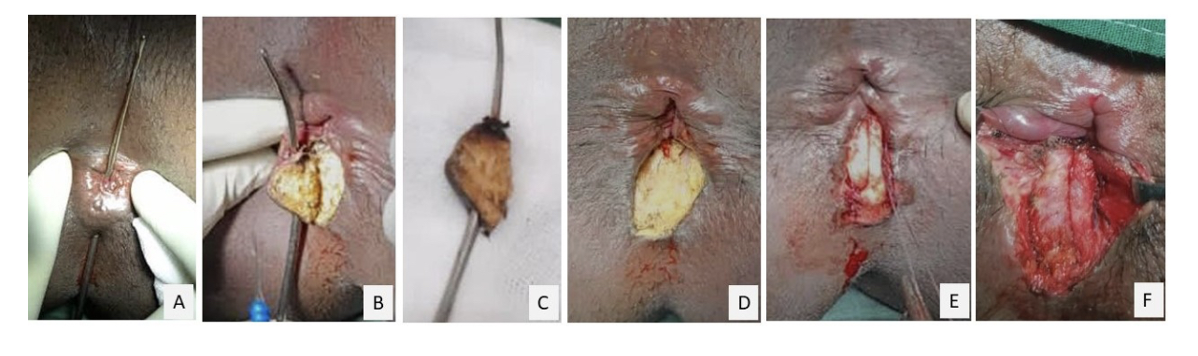
This is a prospective observational study of patients with trans-sphincteric anal fistula who underwent fistulectomy with immediate sphincter repair in a single setting from June 2019 to May 2021 at Kassala Police Hospital, Eastern Sudan. All patients with high trans-sphincteric anal fistula who reported to the surgical clinic were included in the study to avoid selection bias. Exclusion criteria were: 1. Patients who refuse to participate in the study 2. Patients who defaulted follow up 3. Patients with complex or recurrent Fistula-in-ano (FIA). Variable parameters included were demographic data, physical examination, preoperative faecal incontinence score and pre-existing comorbidities such as diabetes mellitus, steroids usage and previous anal surgeries. All the operations were performed under spinal anesthesia with metronidazole as prophylaxis. The patients were placed in lithotomy position, the examination under anesthesia was performed, and the preoperative anal fistula type was confirmed with a digital examination, flushing of the external opening with the diluted hydrogen peroxide to identify the internal opening and a Lockhart-Mummery fistula probe was used to guide fistulectomy. The fistula tract was excised completely using monopolar diathermy along the Lockhart-Mummery probe. The two edges of the divided sphincter were held with Allis grasper, approximated with the interrupted horizontal mattress using Vicyrl 1 (Fig. 1). All the patients followed the same-day care protocol and were discharged on the same day after recovering from spinal anesthesia, careful wound inspection for active hemorrhage, and adequate pain control. Patients were discharged with oral analgesia using paracetamol and diclofenac sodium when needed and regular oral metronidazole for seven days. Outcomes measured were immediate post-operative bleeding, pain score that requires regular analgesia, wound infection, excessive itching, fecal incontinence with Wexner incontinence score, anal stenosis, time to resume normal activities and time to wound healing. The follow-up data were collected up to 24 months after their index surgery. Data were collected prospectively using questionnaire, and patients’ records. Phone calls were used for long term follow up if the patient was well in the initial clinic visits. Data were transferred from an Excel sheet for tablature. All methods were carried out in accordance with Helsinki Declaration and relevant guidelines and regulations. All patients who participated in the study had informed consent from the patient or their legal guardian. The approval to conduct the study was obtained from the Ethics and Research Committee in Kassala Police Hospital
__complete_fistulectomy_(b)__the_fistul.png)
Results
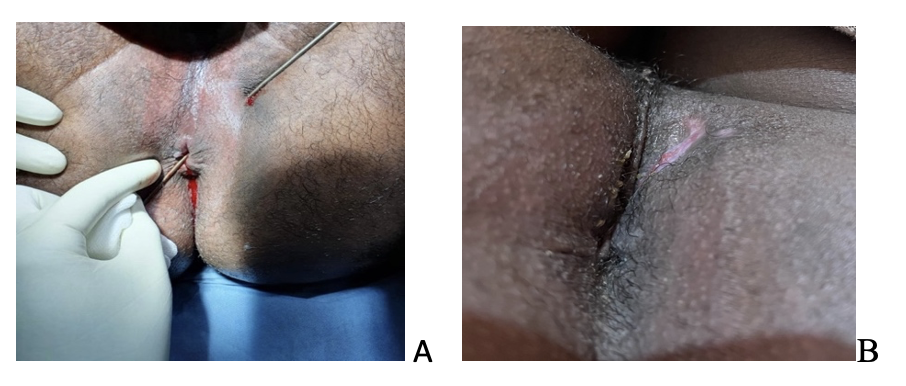
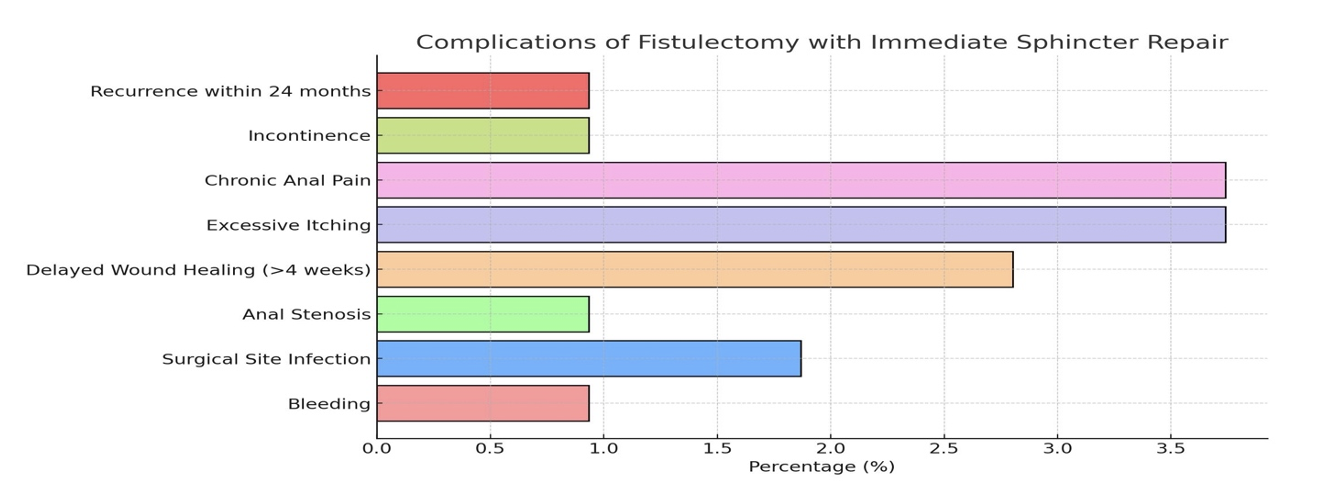
The total number of 212 patients were recruited for this, however, 23 patients refused to participate and choosed other treatment modality, 51 defaulted follow-ups after initial clinic visit and 31 had either complex or recurrent fistulas. A total of 107 participants have complete data and their results were analyzed in this study. The cohort was 74.3% male. Their median age was 40 years old, with a range from 66 to 23 years old. Twelve (11.2%) patients had diabetes, and 8 (7.4%) were on steroids. Seven patients (6.5%) have associated anal conditions with previous anal surgery. The post-operative assessment revealed minor bleeding, which stopped spontaneously on compression in one patient (0.9%); six (5.6%) patients were started on regular analgesia on the operative day (Table 1). During the follow-up, wound infection occurred in two (1.8%) patients, eventually healing within two weeks. 101 (94.4%) of the patients resumed normal daily activities after one week, five (4.7%) patients after two weeks, and one (0.9%) needed three weeks to return to regular normal activities. One (0.9%) patient developed anal stenosis that resolved with a single session of anal dilatation. Chronic anal pain occurred in four (3.7%), while gas incontinence (Grade 1 according to Wexner score) occurred in one (0.9%) patient. Four (3.7%) patients developed excessive itching. The majority had the wound healed within one month, and only four (3.7%) patients needed more than one month for complete wound healing (Figure 2). They were all previously on steroids for other medical conditions including bronchial asthma and rheumatoid arthritis. Fistula recurrence was found in one (0.9%) patient at the 6-month follow-up, and no other recurrence was found within the 24-month follow-up. The incidence of complications and recurrence is illustrated in Figure 3.
__and_four_weeks_after_operat.png)

Discussion
The results of this study evaluating fistulectomy with immediate sphincter repair for high trans-sphincteric anal fistulas highlight a promising balance between high healing rates, minimal complications, and continence preservation. In this cohort, 94.4% of patients resumed normal activities within one week, with minimal complications like minor bleeding (0.9%) and wound infection (1.8%), which aligns well with current literature findings on this surgical technique.The healing rate in our study was high, with only one patient (0.9%) experiencing recurrence within 24 months. This aligns with other studies reporting healing rates between 93% and 95%, depending on factors such as patient selection, procedural specifics, and postoperative care.1,3,4 Immediate sphincter repair appears to maintain fistula eradication while protecting sphincter integrity. Recent literature also highlights recurrence rates generally below 5% in similar cases when treated with sphincter-preserving techniques, particularly for complex trans-sphincteric fistulas, although longer follow-ups can reveal slightly higher recurrence rates.5,6
On comparing fistulectomy with immediate sphincter repair with Seton Techniques, cutting setons, often used for high trans-sphincteric fistulas, are associated with a risk of incontinence averaging 25%, though outcomes vary based on the specific technique used and patient characteristics.7–9 In contrast, fistulectomy with immediate sphincter repair has been associated with incontinence rates as low as 3-9% in recent studies, supporting the preference for this technique in patients where continence preservation is critical. The reduced need for frequent clinical visits, as required by setons, also improves patient satisfaction and reduces chronic discomfort related to wound care.10,11
On reviewing complications and Quality of Life, the study’s low rates of postoperative bleeding (0.9%), wound infections (1.8%), and anal stenosis (0.9%) are indicative of the procedural safety in experienced hands (Table 1). These results are consistent with systematic reviews suggesting that complications following fistulectomy with immediate sphincter repair, when performed by skilled surgeons, remain low, with most wound infections resolving within two weeks.12,13 Additionally, the majority of patients in this study (94.4%) returned to regular activities within a week, showing the benefits of this approach in enhancing postoperative quality of life.14
Chronic anal pain affected 3.7% of patients in this study, a finding that underscores the importance of postoperative management. This pain can persist for months, it has been linked to both the surgical technique and the patient’s pain threshold. Interestingly, patients on steroids experienced delayed wound healing, which aligns with reports that chronic steroid use can impair immune response and tissue repair, suggesting that preoperative management for steroid-dependent patients may be beneficial.7–9,11
Regarding the long-term sphincter function, immediate sphincter repair has been shown to reduce the risk of postoperative incontinence while preserving anal function, with incontinence rates of 12-23% reported in some studies for higher-risk patients.4–6,10 However, gas incontinence (grade 1 Wexner) observed in only one patient (0.9%) in this study,it was mild and resolved with pelvic floor exercises, supporting the utility of adjunctive therapies for optimizing long-term continence outcomes.
Clinical assessment is generally more accurate for simple trans-sphincteric anal fistulas (as in this study) than for complex cases. Simple trans-sphincteric fistulas often follow a predictable course and are easier to palpate, which enhances diagnostic accuracy through physical examination alone. However, even in simple cases, small secondary extensions or abscesses can occasionally be missed, which may contribute to recurrence if not identified. Recent literature supports the use of adjunctive imaging, such as MRI, to confirm clinical findings, as it provides additional detail and can reduce the risk of incomplete treatment. Scholz et al. highlight that even for simple fistulas, MRI can offer valuable reassurance and precision in preoperative planning, though it is often reserved for cases where examination findings are inconclusive.15 Although, our cohort were diagnosed with simple FIA, but this should guide our future projects in anal fistulas field.
The study was conducted at Kassala Police Hospital, located in Kassala, Eastern Sudan. Kassala is a resource-limited region with ongoing conflicts that classify it as a war zone. The hospital operates on a restricted budget and faces significant challenges due to limited resources. It is a secondary care facility with approximately 120 inpatient beds and handles around 1500 emergency visits annually. The surgical cases are predominantly general surgery, as subspecialties and highly trained staff are scarce. Advanced surgical equipment and technologies and specialized surgical tools, are limited. These constraints necessitate reliance on practical and cost-effective solutions, as demonstrated in this study.
Limitations of the study
This is a prospective observational study, which lacks a comparative arm. The study was descriptive due to the small sample size. We did not routinely use imaging such as endoanal ultrasound or magnetic resonance imaging for anal fistula mapping due to financial constraints in our country. All the anal fistula mapping was done with examination under anesthesia using digital examination ,hydrogen peroxide flushing, along with a fistula probe by the colorectal surgeon.
Strengths of the study
A single surgeon performed this study; hence, the technical bias due to the variation of techniques was minimized. The data were collected prospectively, such as the pain score and Wexner’s incontinence score, minimizing the number of missing data for analysis.
Recommendations
Multi-center prospective observational study on the strategies towards high trans-sphincteric anal fistula involving other approaches compared with the fistulectomy with immediate sphincter repair. For future directions, further research could focus on refining sphincter-preserving techniques and optimizing patient selection, particularly for steroid-dependent individuals, to improve both healing rates and continence outcomes. Additionally, potential risk factors for failure of the technique such as obesity, obstetric history, smoking and fistula location should be explored. Expanding sample sizes and increasing follow-up duration will also provide a clearer picture of long-term recurrence and continence rates, which are crucial for evidence-based decision-making in anal fistula management.
Conclusions
Fistulectomy with immediate sphincter repair is a safe, practical and feasible option in treating high trans-sphincteric anal fistula with comparatively good outcomes and acceptable complication rates in a colorectal center in Sudan.
List of abbreviations
FIA: Fistula-In-Ano