
INTRODUCTION
Artificial intelligence describes computational algorithms that can perform tasks typical of human intelligence, especially when processing and analyzing data.1 As medicine embraces digitalization, an abundance of data will be generated both at the individual patient level and on a broader scale across healthcare providers and institutions. In today’s era of precision medicine and personalized health, data-driven evidence will increasingly guide patients and practitioners in making informed decisions. Although lack of access to high-quality data and high-powered analytical tools has hindered medical advancement in the past, rapidly progressing capabilities of artificial intelligence and machine learning, the techniques by which computers and AI undertake complex tasks, now enable clinicians to compare individual patient data across the entire care continuum against millions of related or similar cases.2,3 Additionally, artificial intelligence has made tremendous strides in image recognition, natural speech processing, textual analysis, and self-learning.4 These newly enhanced capabilities could reshape everything from health management systems (i.e. electronic health records) to active guidance of practitioners in treatment plans and patient care.5
The introduction of new and powerful hardware in association with unforeseen data storage capabilities suggests immense potential in cardiac anesthesia across the continuum of patient care. Cardiac anesthesiologists have a significant impact on the quality of care delivered to cardiac patients by implementing anesthesia-specific practices and by participating in team-based care with other clinicians.6 Applications of AI in the field of anesthesiology include depth of anesthesia monitoring, control of anesthesia, ultrasound guidance, pain management, event and risk prediction, operating room logistics, and physician training, however, some applications are more pertinent to cardiac anesthesiology than others.7 For example, AI used to automate and guide echocardiography, a diagnostic tool for intraoperative monitoring and assessment of patients with cardiovascular diseases, is especially beneficial in improving speed and accuracy of image analysis. This could assist cardiac anesthesiologists with accuracy and efficiency of manual tracing, as well as produce more standardized analyses of echocardiographic imaging to mitigate human error.8
In this article, we delve into current and future applications of AI and ML in cardiac anesthesia, discuss future directions, and highlight potential limitations or risks. Our goal is to elucidate the potential role of artificial intelligence in cardiac anesthesia across the continuum of care.
REVIEW
Learning Models
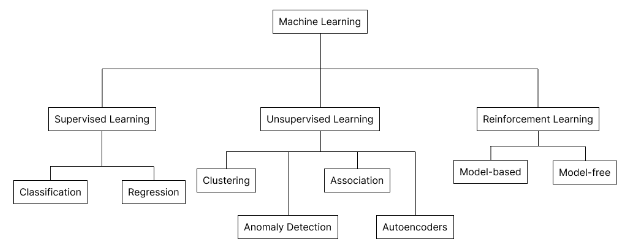
Artificial intelligence has been described as a system that mimics human intelligence processes to effectively improve, optimize, or automate a task or problem. AI encompasses several sub-fields including advanced statistical modeling, deep learning, and machine learning.9 Machine learning is best described as the method by which computers perform specific tasks by studying patterns in the data, without being explicitly programmed for that purpose. ML is usually categorized as supervised learning, unsupervised learning, and reinforcement learning (Figure 1).10

Supervised learning describes having a full set of labeled data, indicating the data is tagged with the answer the algorithm should produce on its own, while training an algorithm. This is particularly useful in classification problems and regression problems, for example classification of animals in a pre-labeled dataset of animal images or creation of predictive regression models for apartment prices based on square footage.
Unsupervised learning describes having an unlabeled dataset without instructions when training an algorithm. In this case, the neural network, a computational model that transforms input data and learns through multiple transformations, seeks to identify structure in the data marked by detectable features. Methods of data organization in unsupervised learning include clustering, anomaly detection, association, and autoencoders. Clustering works by identifying and grouping similar data together. Anomaly detection works by flagging outliers in the dataset. Association works by correlating features of data with other features to predict commonly associated attributes. Autoencoders attempt to generate summarized code from existing input data, but this is generally not useful in real-world applications of unsupervised learning.
Reinforcement learning describes AI agents that find the optimal way to complete a task or goal by learning from past feedback and new tactics to receive a reward. The goal of the AI agent is to maximize the reward. Reinforcement learning is often the method by which robots are trained.11
Growth in Medicine
Many practices including electrocardiogram readings, white-cell differential counts, and cutaneous lesion analysis have long relied on machine learning to eliminate the risk of human error. However, recent technological advancements have facilitated a path for artificial intelligence and machine learning to pervade every aspect of medicine and patient care, including infectious disease identification, diagnostics, clinical decision-making, and research.12 From supervised learning models being used to study blood pressure data to auto-normalization of anatomical phrases in radiology reports using unsupervised learning, the applications of ML in medicine are vast.13,14 Anesthesiologists, whose jobs consist of perioperative and intensive care, pain management, drug delivery, and drug discovery, could greatly benefit from advances in AI and ML.15
Most publications on AI in medicine were published in the last 5 years.3 By June 2023, there were 2,548 results on PubMed when filtered for text words “AI” and “anesthesiology”. As the popularity of AI increases in the medical community, there will be associated implications for the workforce. While the introduction of AI and ML in patient care is changing the job description of many medical professionals, we are a long way from complete job replacement. Physicians and other clinicians use a holistic problem-solving approach that incorporates logic and human emotion to arrive at reasonable conclusions, a skill AI has yet to master.16
As far as its economic potential in medicine, it is estimated that wider adoption of AI could result in savings of 5 to 10 percent in US healthcare spending based on data from models using existing AI technology.17 AI-based systems are closely associated with the Internet of Medical Things (IoMT), a proposed interconnected network of physical objects integrated to exchange data between devices using the internet.18 The IoMT, artificial intelligence, machine learning, and deep learning are all key factors in developing a more efficient and cost-effective health ecosystem.19
Continuum of Care
Cardiac anesthesiology, a subfield of anesthesiology, has historically emphasized the importance of intraoperative care.20 Recently, findings suggested equal focus should be directed towards advancements well into the preoperative and postoperative periods of care.21 The spectrum of responsibilities of an anesthesiologist, aside from prevention of intraoperative death, include complication reduction, trauma mitigation, patient recovery, and overall efficiency. The preoperative evaluation is an essential component of the anesthesia continuum of care. It allows an anesthesiologist to determine perioperative risk, as well as investigate the patient’s condition as it pertains to the challenges of surgery and recovery. High-quality preoperative care is characterized by an efficient experience for patients in association with adaptability in circumstances of uncertainty. Postoperative care responsibilities of an anesthesiologist primarily include organizing appropriate critical care resources and managing pain and suffering.22
Preoperative Applications
Perioperative morbidity and mortality of cardiac surgery patients rely heavily on the patient’s preoperative condition and postoperative complications, including factors such as age, sex, type of surgery, history of cardiac disease, and urgency of surgery.23 Typically accounting for a variety of factors, risk models attempt to mathematically calculate scores to gauge the preoperative risk of a cardiac patient. Frailty, heart failure, kidney and liver function, nutritional status, pulmonary disease, diabetes mellitus, preoperative anemia, medication regimen, and imaging are among the factors that should be considered in a preoperative evaluation.24 The ability of AI/ML to aggregate and analyze massive amounts of data to assess the preoperative state of a patient significantly enhances traditionally limited risk models. AI and ML models automate computational analysis of large datasets and compare the weighted effect of labeled inputs (i.e. age, sex, lab values) to the desired output. Current studies note the added value of advanced machine learning models in prediction of mortality in elderly and rheumatic heart disease subpopulations, as well as in risk survival scores in heart transplantation patients.25 As the capabilities of AI continue to grow, models that predict mortality risk, cardiac risk, pulmonary risk, risk of acute kidney injury, and other complications will become increasingly accurate and efficient.26
Existing literature extensively details how AI uses algorithms to decipher complex data and accurately analyze diagnostic imaging. The focus of AI, especially in fields that rely on medical imaging such as cardiac anesthesiology, has been on detection, quantification, and qualification of numerous clinical situations.27 One such example involves preoperative cardiac evaluation with echocardiography, often performed before noncardiac surgery.28 AI applications in echocardiography optimize three-dimensional image analysis and speckle tracking to create comprehensive and organized data analyses for anesthesiologists.8 These AI/ML solutions have already been applied to automate measurement of left ventricular ejection fraction (LVEF), chamber dimensions, and wall thickness.29–31 Although expert anesthesiologists may be able to accurately classify images, complex pattern recognition in big data is better suited for machine learning and AI-based cognitive tools for automated analysis.32
Intraoperative Applications
The intraoperative responsibilities of a cardiac anesthesiologist include monitoring the patient for complications and obtaining/analyzing medical images. In terms of patient monitoring, clinicians often manage hemodynamic status and unexpected intraoperative complications.
Four out of five hemodynamic warnings in cardiac surgery are false alarms for which therapeutic intervention is unnecessary.33 This inaccurate alarm system poses a significant distraction, sometimes referred to as alarm fatigue, in cardiac surgery.34 With its advanced capabilities in predictive analytics, AI and ML models have the potential to predict hemodynamic stability to effectively reduce the rate of false alarms and identify real issues.35 The incidence of hypotension, a potential hemodynamic complication during cardiac surgery, is predicted using an advanced logistic regression-based model that was trained with an exceptionally large dataset.36,37 Additionally, tools such as the Pulse Indicator Continuous Cardiac Output (PiCCO) system take advantage of machine learning to offer anesthesiologists less invasive methods by which hemodynamic status can be monitored.38
Aside from patient monitoring, cardiac anesthesiologists perform echocardiography and ultrasound procedures that require classification and analysis of medical imaging. AI can be used to generate automated interpretations of echocardiograms, thereby reducing the risk of human error.39 For example, current studies highlight machine learning and deep learning models that have shown feasibility and accuracy in measuring LVEF and global longitudinal strain in echocardiography.40 There are a few different applications of AI for ultrasound automation in cardiac anesthesia. One application is ultrasound guidance, where AI is used to assist clinicians in obtaining more objective and precise measurements during ultrasound imaging, removing a significant barrier to practice for several less experienced anesthesiologists.41 AI-powered ultrasound has drawn comparisons to the safety and clinical efficacy of the PiCCO system when used to assess critically ill patients.42 Given that AI has the power to complete image enhancement and analysis, it can make great contributions to the automation of cardiac imaging, MRI, ultrasound, echocardiography, and cardiac CT.43
The most common need for AI in clinical decision-making as it pertains to cardiac anesthesia is optimization. By infusing dobutamine to routine off-pump coronary artery bypass grafting patients during cardiac displacement, AI models optimize cardiac output and improve thoracic aortic blood flow.44 Furthermore, studies have found that AI has been shown to optimize intraoperative blood component utilization in cardiac surgery by employing effective auditing methods to relay useful feedback to anesthesiologists.45 In terms of anesthesia administration and maintenance, AI algorithms are used to ensure optimal dosing, as well as to maintain continuous administration using real-time patient data.46 This is mainly possible due to the unforeseen event and risk prediction powers of modern AI models. It is evident that intraoperative anesthesia care stands to benefit the most from advances in artificial intelligence and machine learning.
Postoperative Applications
Postoperative care in cardiac anesthesia is a vital component of facilitating patient recovery and managing potential postoperative complications. AI algorithms can be especially beneficial in optimizing pain management and monitoring patients postoperatively.
Currently, AI and ML technologies assess and manage pain in a patient-focused manner, both in terms of measurement and prevention.47 As emphasis on precision medicine continues to grow, pain management will become more specific to a patient’s subjective pain tolerance, resulting in the utilization of AI to offer more targeted intervention than previously offered.
Considering the physical and mental stress of cardiac surgery, cardiac anesthesiologists typically must monitor patients very closely following the operation. In terms of immediate postoperative care, optimizing cardiovascular function with purposeful hemodynamic therapy can decrease morbidity and duration of hospital stay.48 A common postoperative complication is hypertension, a condition that can easily be tracked and predicted by high-powered AI.49 While hemodynamic complications are the most common, other issues such as delirium can also cause patients to suffer postoperatively. While there is no current method by which delirium is detected and prevented postoperatively, current technology indicates the potential for AI to predict onset and severity.50 ML algorithms use concepts of supervised learning in which the desired output is known. Therefore, postoperative care is the cardiac anesthesia continuum of care period that can most easily be made more efficient.
Future Directions
The future of artificial intelligence and machine learning in cardiac anesthesia is exciting and presents new opportunities to advance the field of anesthesiology entirely. The integration of AI across the continuum of care will become more popular, and continued advancements in software and technology will lead to further improvements in cardiac anesthesia.51,52 Applying AI to mundane tasks will afford anesthesiologists more time to dedicate towards effective patient care and care delivery. Automation of documentation, billing, coding, and image analysis provide an unprecedented convenience to clinicians while reducing operational costs of the overall facility.
While current models of AI are intelligent, we have only scratched the surface in terms of its potential intelligence and capabilities. As it stands, AI is capable of mimicking human intelligence and incorporating human intelligence into computer functions, but the most current AI technologies still fall short of human intelligence.53 These advanced algorithms have made significant progress in areas of natural language processing (NLP), computer vision, speech recognition, robotics, and autonomous systems.54 These growing capabilities will fill gaps in clinical safety and information security in the coming decades.55 From using machine learning models to track and analyze procedures to creating cybersecurity models to protect patients from HIPPA violations, the medical field will undergo a noticeable transition to the era of digital medicine. In April of 2023, the electronic health record company known as Epic announced its intention to integrate AI into Epic software to harness large-scale data analysis capabilities within a full hospital network’s system.56 Moreover, AI will simultaneously pervade other fields of science. For example, AI integration in materials sciences will optimize development of composite materials for anesthesiology procedures.57
One proposed future is an interconnected ecosystem fully integrated with highly intelligent AI and ML algorithms that use our real-time medical information to formulate and execute all-inclusive, efficient health plans. The Internet of Medical Things (IoMT) and AI will be technologies that work collaboratively to enhance healthcare systems and revolutionize patient care (Figure 2). The combination of AI and IoMT, known as Artificial Intelligence of Things (AIoT), will continue to support more healthcare processes as artificially intelligent devices gain connection to the internet.58 As the industry blossoms and empowers devices to capture immense amounts of data, key leaders in anesthesiology and medicine must advocate for proper routes of implementation. If used correctly and ethically, patients of previously fatal conditions could face a different reality in a matter of months. It is the duty of medical professionals to seek more cost-effective, patient-centered solutions within patient care and understand how applications of artificial intelligence may optimize or facilitate that solution.
_and_ai_will_be_technologies_that_work_collaborativel.png)
Limitations
While the main value proposition of AI is its data aggregation and analysis capabilities, the amount and type of data available is often the limiting factor in the efficacy of the algorithm. AI systems require tremendous amounts of data to generate accurate predictions, but that data could be scarce or biased.59 This issue is compounded by the need for fast computational speeds, high data transfer rates, and immense data storage to sustain an effective AI model.60
Major challenges in AI as they pertain to medicine lie in the ethics of using artificial intelligence and the need for sufficient training of clinicians.61,62 In terms of ethical considerations, the difficulty in interpreting AI poses a mistrust in the knowledge it provides, thereby hindering informed decision-making for patients and practitioners.63 In today’s technology-driven society, there is a significant ethical concern with privacy and anonymity, especially with the growing popularity of AI.64 This steady growth will call for legislation to build regulations and ensure fairness, privacy, and morality. There have already been efforts to develop comprehensive risk-based regulatory approaches to AI, with the recognition that medicine is a high-impact sector.65 Currently, different regions have posed vague and contradictory regulations, and this lack of a universal system is one potential limitation to ethical implementation of AI.66
Aside from privacy concerns, training physicians on all aspects of AI is unreasonable so developing plans to educate clinicians on effectively using AI to increase job efficiency is crucial.67 Currently, most established practitioners are relatively unaware of the full capabilities of AI, however, medical schools have been advised to begin including AI education in their curriculums.68 As we move forward, the medical education system should provide methodical training in AI techniques and methods to develop physicians’ roles as information aggregators, consultants, and patient supporters.
CONCLUSIONS
Artificial intelligence and machine learning have proven to be essential in predicting risk, optimizing clinical management, and promoting personalized care. While challenges such as algorithm bias and clinician training currently remain, AI presents itself as a tool in cardiac anesthesia to create efficient, patient-centered solutions while maintaining the highest standards of safety and accountability. This review highlights the vast potential of artificial intelligence and machine learning across the perioperative continuum and calls on cardiac anesthesiologists to adapt to the evolving landscape of digital medicine.