Introduction
Immune-checkpoint inhibitors (ICIs) have transformed the landscape for cancer treatment by enhancing the endogenous immune system’s ability to eliminate cancer cells. Though formally recognized in 2011 with the creation of the first ICI, ipilimumab, it was William Coley, known as the “father of immunotherapy,” who first attempted to treat bone cancer in 1891 via activation of the immune system. Since 2011, ICI use has delivered promising clinical breakthroughs and revolutionized the standard-of-care approach in the treatment of various cancers. The estimated percentage of patients with cancer who were eligible for ICI use increased from 1.54% in 2011 to 43.63% in 2018. Currently, over 230,000 patients are prescribed ICIs annually in the US alone. They now have the ability to act in several adjuvant and combination regimens as opposed to single-agent immunotherapies. Despite producing astonishing improvements in prognosis and remission-free time frames for cancer patients, ICI’s carry risks for well documented treatment-related complications and immune-related adverse events (irAEs). As ICI usage increases, patients who experience these side effects will increasingly present to the Emergency Department. Thus, it is crucial that emergency medicine clinicians have insight about these medications, their adverse effects, and management options.
Mechanism of Action
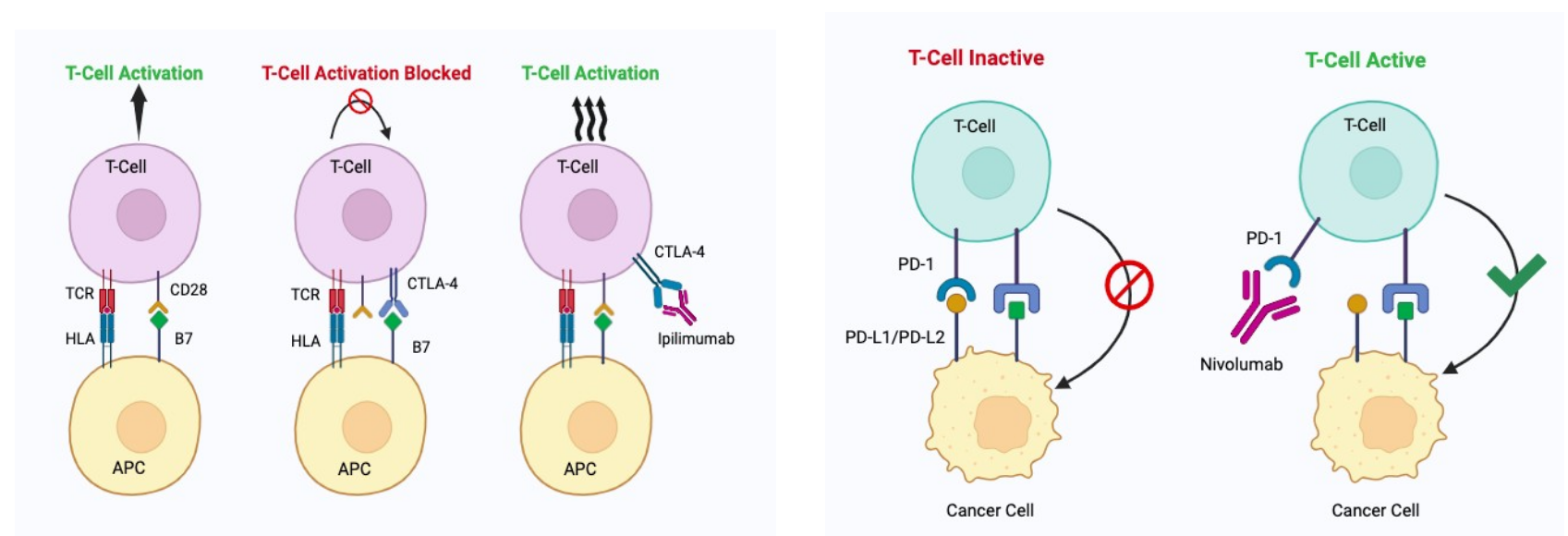
The mechanism of action of Immune checkpoint inhibitors is based on a recognition that cancer cells spread, in part, by actively downregulating the host immune system (which would otherwise recognize and eliminate cancer cells). Tumor cells evade immune response by blocking T cell activation. ICIs function by blocking this inhibition, thereby boosting the immune system’s ability to kill tumor cells. In comparison, conventional treatments like chemotherapy, hormonal therapy, or targeted therapy work by interfering or diminishing cancer signaling pathways, cell division, and DNA synthesis. ICIs offer a more targeted and adaptable attack specific to the tumor cells, with the added advantage that T cells display memory for these cells in cases of recurrence or metastasis. T cells contain co-stimulatory and checkpoint proteins that can be altered by various agents, which in turn affects their ability to target cancer cells. These agents activate T-cells by either turning on co-stimulatory proteins or blocking checkpoint proteins. Though they regulate immune responses using different mechanisms, CTLA-4 and PD-1 were two of the first checkpoint proteins targeted to enhance T cell function.

Ipilimumab and Nivolumab were two of the first immunomodulators to gain FDA approval, and are among the two most common ICIs being used today. Ipilimumab, an Anti-CTLA-4, functions by counteracting the ability of CTLA-4 to diminish the costimulatory receptor of CD28, thus allowing cytotoxic lymphocytes to continue destroying cancer cells. Nivolumab, on the other hand, blocks activation of the programmed cell death 2 (PD-1) receptor on T cells, therefore releasing the brakes on the immune system and allowing proliferation of T cells. Some of the hallmarks making this immunotherapy unique are long-term survival benefits, improved health-related quality of life, and unique safety profiles.
By 2023, eleven checkpoint inhibitors had been approved for 18 different indications, with at least one being approved to treat any type of solid organ tumor as long as it shares specific molecular characteristics. Given its rapid acceleration into the oncologic world, we can expect ICI use to increase dramatically as potential combinations of therapies are created.
Adverse effects
Despite their impressive efficacy, ICIs come with the cost of inflammatory toxicities, especially when therapies are combined. Immune Related Adverse Events (IrAEs) are considered off-target effects when an immune system is excessively activated, especially in the case of ICIs, which promote T cell expansion and activation. A thorough understanding of these serious side effects will enable providers to optimize treatment plans, especially for emergency medicine physicians, who will often be the front-line provider when most of these irAEs arise. IrAEs can occur in almost any organ system, and although they usually occur early in treatment, typically within the first three months, they can occur up to several months after treatment has ended.
Some common complications involve the cutaneous, gastrointestinal tract, pulmonary, and endocrine organ systems:
Cutaneous: Cutaneous irAEs occur between one-third and more than half of all patients receiving ICIs, with rash, pruritus, and vitiligo being the most commonly reported symptoms.
Endocrine: Endocrine abnormalities including adrenal insufficiency, mild thyrotoxicosis, and primary hypothyroidism are also associated with ICI use.
Gastrointestinal: Colitis occurs at a rate of 10-20% in patients receiving ipilimumab, and is the most common irAE seen in this patient population.
Pulmonary: Pneumonitis is a life-threatening iaRE, and is prevalent at a rate of 1-5% in patients receiving anti-PD-1 antibodies, compared to <1% in patients receiving anti-CTLA-4 antibodies.
Cardiac: ICI-induced-myocarditis occurs at a rate of 1.14%.
Up to 60% of patients treated with ipilimumab (an anti-CTLA-4 medications) had an irAE of any grade throughout their treatment course, with up to 30% of those being grade 3 or higher. In comparison, patients taking anti-PD-1 medications (such as nivolumab or pembrolizumab) encounter less frequent grade 3 irAEs (~10%). A phase II trial revealed that in patients receiving combined treatment (ipilimumab plus nivolumab), incidence of grade 3 toxicities occurred at 54%, compared to 24% in patients receiving ipilimumab alone, highlighting that these medications in combination often increased not only incidence, but severity, of irAEs.
Emergency Department Management ICI related adverse effects
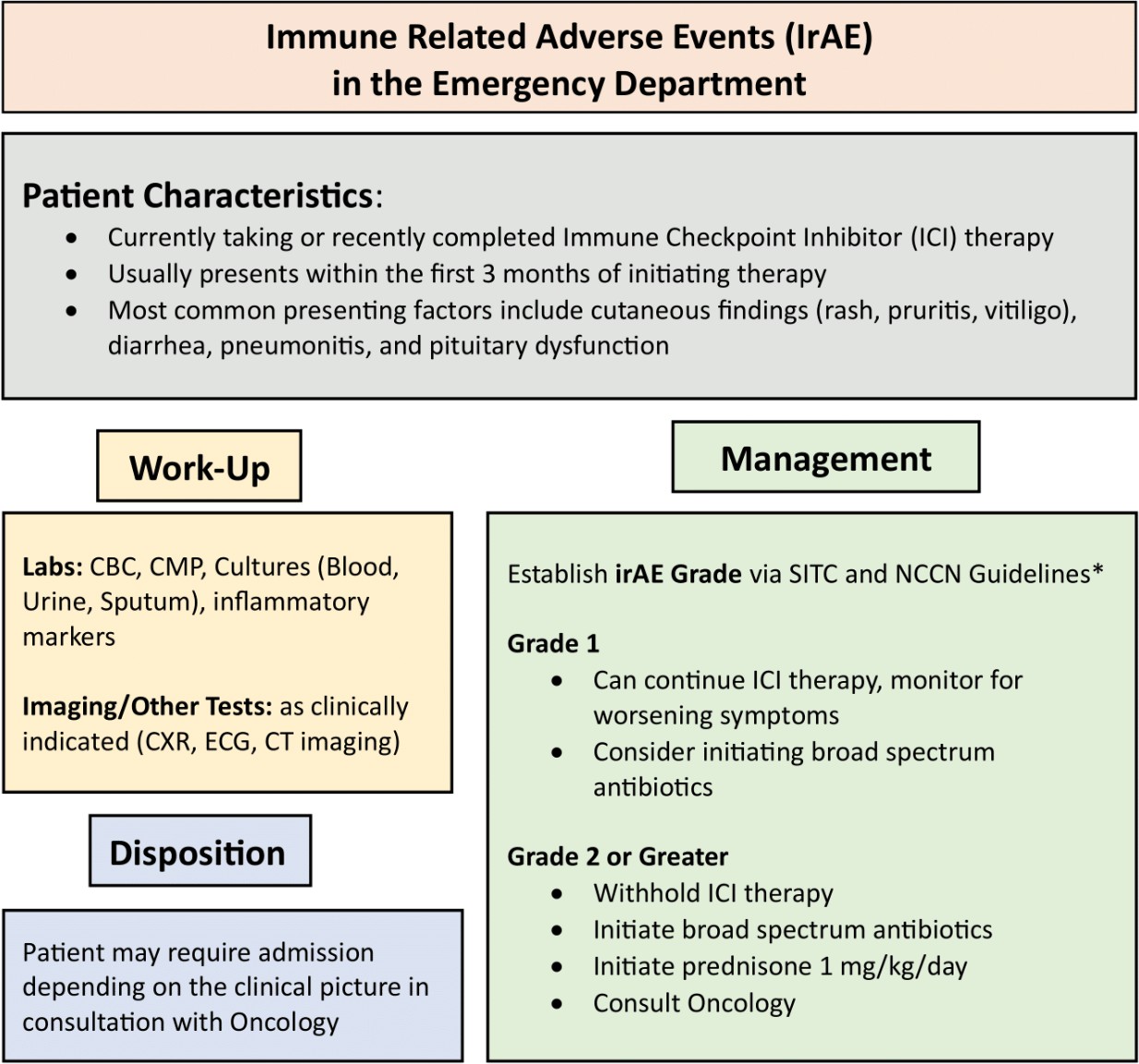
Guidelines outlining the general treatment algorithms for irAEs have been published by the Society for Immunotherapy of Cancer (SITC) and the National Comprehensive Cancer Network (NCCN). Despite organ-specific management with certain irAEs, there are some generalized overarching principles when it comes to managing irAEs. When patients present with symptoms consistent with irAEs, a rigorous and thorough infectious work-up is usually required, commonly through blood cultures, biopsy samples, and Clostridium difficile testing. Another reason to pursue full clinical work-ups includes asymptomatic biochemical abnormalities (ex. electrolyte abnormalities, elevated serum creatinine, etc). Once the grade of the irAE is assessed, treatment can begin, and typically includes immunosuppression with corticosteroids, symptomatic treatment, and/or discontinuation of the ICI depending on the grade and severity of presentation.
Per the SITC clinical practice, grade 2 irAEs or higher should have ICI therapy withheld and prednisone should be started at a dose of 0.5-2 mg/kg/day. Patients should be counseled about potential toxicities when starting this therapy. This is considered an emergent intervention, as controlling an overactive immune response early could allow patients to resume this life-saving medicine down the line, should their ICI be held. Decisions about holding ICI therapy depends on the grade of the irAE: grade 1 irAE can be continued but should be monitored for worsening symptoms, grade 2 should have ICI therapy temporarily withheld. Benefits and risks need to be thoroughly considered when deciding to re-challenge patients with ICIs, though these conversations will often require an oncologist and a specialist.
In the Emergency Department, the priority for providers will be to rule out other infectious and dangerous etiologies and to start immunosuppression sooner rather than later. In our practice, when patients on ICIs present with potential ICI related side effects, we begin by initiating a broad infectious workup. After cultures and appropriate infectious labs are drawn, we initiate broad spectrum antibiotics empirically, pending results. In addition, we initiate a 1mg/kg prednisone daily dose to cover for possible irAE, and we have the patient stop further doses of their ICI for the time being. Once the patient has been covered for both infectious and irAE pathology, we encourage consultation and discussion with the treating oncologist to discuss disposition and follow up. While clinicians may be hesitant to start steroids in a patient with potential infectious symptoms, in our experience, oncologists display a low threshold to initiate steroids in these patient populations as long antibiotics have been initiated.

Discussion
A retrospective review done on patients on ICIs who presented to a tertiary care ED between May 2017 and April 2018 found IaREs in 16 (16.3%) of the 98 ED visits, with the most common irAE being colitis (56.3%). That being said, only two (12.5%) patients with irAEs received corticosteroids during their time in the ED. Additionally, only 14.3% of EM providers documented an irAE in their differential diagnosis, despite an irAE ultimately being diagnosed in 43.8% of visits. This study highlights the gaps in knowledge that Emergency Medicine physicians currently have regarding ICI use and their potential adverse effects. Given the expansion in ICI use and the benefits of corticosteroid initiation, early recognition and management of irAEs among ED providers, in conjunction with treating oncologists, are imperative to improve patient outcomes in the Emergency Department.