
Introduction
Acute aortic dissection is an emergent cardiovascular pathology caused by separation of the layers of the aorta and the resulting collection of blood between these layers.1 Prompt diagnosis of this condition is required as it can be fatal without intervention. There are two principal classification systems used for aortic dissections. The DeBakey classification, which utilizes the site of the intimal tear and the Stanford classification that is based on whether or not the ascending aorta is involved.1 We use the Stanford classification in this report. The Stanford type A aortic dissection includes the ascending aorta, the aortic arch, and the descending thoracic aorta while the type B dissection involves the descending aorta.2
Risk factors for aortic dissection include male sex, increased age, pregnancy, genetics, bicuspid aortic valve. Modifiable risk factors include hypertension, dyslipidemia, aortitis which can be either infectious or noninfectious, obstructive sleep apnea, fluroquinolone use, cocaine use, and aortic dilatation.3 Connective tissue disorders such as Marfan and Ehler-Danlos syndrome increase risk of dissection by causing innate weakness in the wall structure.1 Identifying these factors in the emergency department play an important role in early identification of the disease.
Genetic correlation in aortic dissection has been studied to an extent. About 20 percent of the first-degree relatives of those with aortic pathology are affected. Positive family history increases risk of aortic dissection at an earlier age as well as the probability of needing surgical treatment.4 There have been multiple genes that perpetuate risk for aortic aneurysms and dissection. The majority of these studied genes affect either the elastin-contractile unit (ECU) of the aorta or transforming growth factor beta (TGFβ) signaling.5 Genetic correlation is exemplified in this case report specifically.
Complications of aortic dissections are typically due to lack of perfusion. Commonly, cardiac complications are seen. These include aortic regurgitation and congestive heart failure. There is potential for neurologic damage due to prolonged hypotension and/or nerve compression from expansion of the false lumen.1 Diagnosis and early intervention helps decrease these life-altering consequences.
Treatment is typically dependent on the type of aortic dissection present. Characteristically, type A dissections are handled surgically, however individualized approaches should be taken. Type B dissections are more often handled conservatively with risk factor modification as well as strict blood pressure and heart rate control.1
Case Report
Ethical Considerations
The patient provided written informed consent for publication of this case report.
Case Presentation
This is a 66-year-old male with no known past medical history who presents to the emergency department via Emergency Medical Services (EMS) as a ‘trauma activation.’ The patient was working out at the gym when he experienced sudden, severe upper back/neck pain and subsequent loss of sensory and motor function to bilateral lower extremities. The patient was reportedly utilizing one of the gym’s back-specific machines. He arrived to our emergency department’s trauma bay via ambulance. The patient was alert and phonating with a GCS of 15 upon arrival. The trauma alert was downgraded as lack of trauma disqualified the patient from our institution’s trauma criteria. The patient was placed in an ED bed and urgently evaluated at the bedside.
Initial vital signs revealed blood pressure of 114/44 mmHg, pulse rate of 55 bpm, respiratory rate of 26 breaths/min, and an oxygen saturation of 98% on room air. Rapid assessment revealed a moderately-distressed patient with an intact airway, bilateral breath sounds to auscultation, tachypnea, and intact peripheral pulses. He was placed on a cardiac monitor and continuous pulse oximetry. We also placed a cervical collar. Electrocardiogram (EKG) showed sinus bradycardia with nonspecific ST segment changes. No prior EKGs were available for comparison. He was found to have no motor function or sensation to painful stimuli below the level of approximately T8. Back exam displayed no obvious trauma. He did endorse generalized pain with palpation of the thoracic region.
The patient received 5 mg of intravenous diazepam for agitation. The initial plan was to obtain emergent MRIs of the cervical, thoracic, and lumbar spine evaluating for possible pathologic fracture. The radiologist was contacted via phone and approval was obtained for these scans.
Point of care labs obtained were significant for an elevated lactic acid of 4.3 mmol/L, glucose of 107 mg/dL, CO2 of 16.2 mmol/L, hemoglobin of 13.9 g/dL.
The patient’s wife and daughter soon arrived to the bedside. They were able to tell us that the patient had a history of unspecified prostate issues. The daughter also added that she personally had an aortic dissection two years prior that was diagnosed and surgically repaired at our facility. With our patient’s somewhat unusual presentation and this piece of familial history, we placed the order for an emergent CT angiogram of the chest.
Shortly thereafter, the patient became increasingly agitated. His speech became unintelligible and he was attempting to remove his cervical collar. He was unable to be settled with passive interventions and ultimately was given a dose of Benadryl and Droperidol. Unfortunately these were ineffective. The decision was made to intubate the patient for facilitation of his emergency department workup. Rapid sequence intubation with ketamine and rocuronium was performed successfully. He was placed on a fentanyl and propofol drip following the procedure and placement of the endotracheal tube was confirmed by chest x-ray.
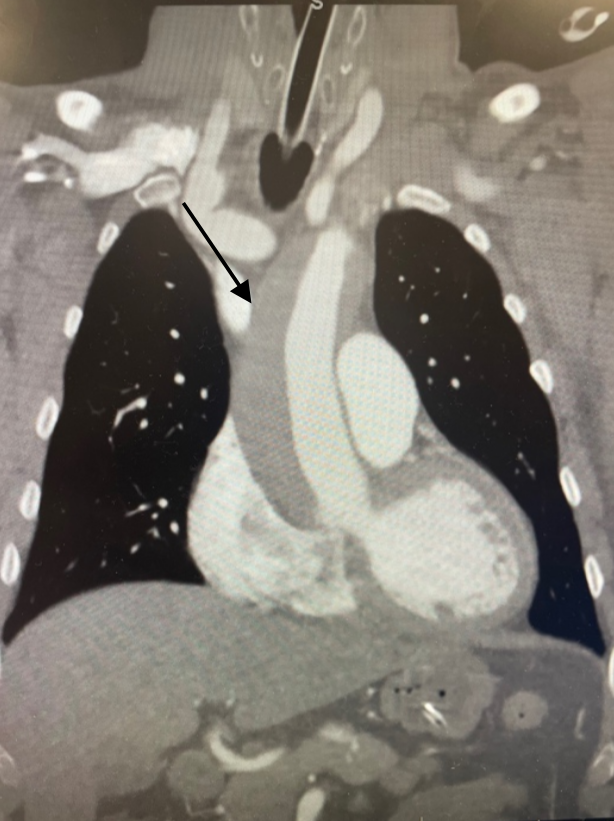
Patient CT angiogram of the chest revealed a type A thoracic aortic dissection that extended throughout the entire ascending and descending thoracic aorta and into the proximal abdominal aorta. The radiologist called with these results and we then placed an emergent consultation to our facility’s cardiothoracic surgery team. After speaking with the surgeon over the phone, plan was made for the patient to urgently go to the operating room for repair. MRIs were then canceled.
.png)
.png)
Vital signs, specifically heart rate and blood pressure, were monitored closely throughout the patient’s ED stay. He did become hypertensive after returning from CT scanner and was initiated on an IV esmolol drip.
In the operating room, patient had a Bentall procedure aortic root replacement with cannulation and repair of the right axillary artery. Patient tolerated the procedure well and was transferred to the surgical intensive care unit in stable condition. Unfortunately, patient had continued lower extremity motor weakness. MRIs of the thoracic and lumbar spine were completed on post-operative day 8, which revealed a syrinx at the level of T8/T9 as well as hyperintense signal in the central conus medullaris suspicious for spinal cord ischemia. These findings were likely caused by occlusion of the artery of Adamkiewic or the segmental arteries that supply the spinal cord.
Conclusion
This case represents and interesting presentation of a type A aortic dissection that also had a familial tie. This case also displayed an example of a neurologic consequence that can occur from severe disease. The patient’s daughter was pregnant at the time of her dissection, so she possessed the risk factors of hormone production as well as genetics. It does seem reasonable to emphasize family history when interviewing patients with any symptoms concerning for aortic pathology. Utilizing the family history, we were able to come to a diagnosis sooner and get the patient to the operating room where definitive treatment was achieved.
Discussion
Thoracic aortic aneurysms remain a life threatening condition that emergency medicine physicians encounter daily. They typically are asymptomatic until an acute rupture occurs that may cause rapid and significant effects on the cardiac system. Early detection remains a challenge as everyone is not routinely screened. Prevalence of aneurysms, dissections, and sudden death is higher for those with first-degree relatives with thoracic aortic pathology necessitating surgical repair.6 Screening should be discussed and recommended to these individuals. Increasing awareness of the disease and its genetic correlation can easily be accomplished by the emergency physician. Additionally, studies have shown that the growth rate of aortic aneurysms is increased in familial versus sporadic cases.6 This could explain the earlier presenting age of acute dissections in familial cases. In the emergency setting, family history should certainly be obtained for all patients presenting with symptoms concerning for aortic pathology.