
1.0. Introduction
1.1. Background
Postoperative nausea and vomiting (PONV) is a common condition among anesthetic patients, manifested clinically by nausea, vomiting, and retching in the first 24 hours after surgery. It is a frequent postoperative complication with debilitating impacts, such as excruciating pain that lowers patient satisfaction and extends patient’s stay at the hospital.1 The severe effects associated with the PONV lead to unplanned readmissions that place a significant financial burden on the family members. In addition to these negative effects, Unsal et al. posited that PONV may result in other problems, including higher medication costs, severe bleeding, aspiration pneumonia and electrolyte imbalance.2 Countermeasures to control and manage postoperative nausea and vomiting following general anesthesia are fundamental to promoting high-quality recovery and patient satisfaction after surgery.
Although the world has made considerable efforts to reduce anesthesia-related nausea and vomiting, such as using antiemetic drugs or implementing non-pharmacological interventions, PONV’s prevalence among the general population remains extremely high. About 75 million patients receive anesthesia worldwide each year, with an estimated 33% developing PONV.3 Teshome et al. found that around 20-50% of anesthetic patients develop PONV, and this prevalence increases dramatically to 80% among patients with high-risk factors such as, the type and duration of surgery, age, sex, prior history of PONV, smoking status, history of motion sickness, etc.4 These findings were justified by Chen and Chang, who reported that PONV is the most common postoperative condition.5 For patients who have undergone craniotomy, the incidence rate of PONV can rise to 50% and 80% for patients with high-risk factors.5 Qian et al. found that female gender, the presence of postoperative pain, and an operation time greater than one hour substantially increase the incidence of PONV after an ambulatory surgery.6 Hence, reducing postoperative pain, as well as operation time, are fundamental methods of reducing PONV following an outpatient surgical operation. Even though antiemetic drugs are widely accepted in managing and preventing PONV, their effectiveness differs due to different factors as outlined above, emphasizing the need for a systematic review to guide clinical decisions and enhance patient outcomes.
1.2. Objective
-
To demonstrate the efficacy of antiemetic drugs in managing and controlling PONV complications after surgery.
-
To compare the efficiency of existing antiemetic medications in managing PONV complications following a surgery.
2.0. Methods
2.1. Protocol and Registration
The research was conducted according to PRISMA guidelines.7 The study adheres to the systematic literature review (SLR) protocol introduced by Kitchenham and Charters who stated that the method consists of three primary stages: (1) planning the SLR, (2) conducting the research, and (3) reporting the outcomes.8 The phases also comprise the following tasks: explaining the inclusion and exclusion criteria, documenting a feasible search strategy, developing the resulting study process, data extraction, and synthesis of the outcomes.
2.2. Eligibility and Criteria
The systematic review included articles that met the following criteria: cohort studies and randomized control trials (RCTs) evaluating pharmacological interventions for managing PONV, studies with the adult patient population (above 18 years), studies where patients underwent surgery after taking antiemetic medication in the preoperative phase, and RCTs that compare the efficacy and severe effects of single or multiple doses of antiemetic drugs. The systematic review included all the studies that have examined the effectiveness of one or more classes of antiemetic medication, including receptor antagonists, such as 5-HT3, D2, and NK1, or antihistamines, corticosteroids, and anticholinergics. Further, only full-text articles and those published in English were eligible for this study. The review omitted all abstract publications and studies older than five years. A general rule of thumb in medical and scientific research is to utilize resources that are not older than five years to avoid the problem of outdated information. Consequently, this explains why January 2020 was selected as the search date. Additionally, the exclusion criteria omitted all the studies that do not explicitly evaluate the effectiveness of antiemetic medications.
2.3. Information Sources
As already described, the information for this study was retrieved from PubMed, Google Scholar, and Cochrane Library databases. Searching information from multiple databases was critical for optimal identification of all literature related to antiemetic drugs and their benefits in ameliorating the severe effects of PONV complications.
2.4. Search Strategy
Information for use in this study was searched from PubMed, Google Scholar, and the Cochrane Database of Systematic Reviews (Ebsco) for studies published after January 2020 to avoid the problem of outdated information. The literature search combined both free words and MeSH terms, including “PONV” (such as “postoperative nausea and vomiting,” “postoperative vomiting,” and “postoperative emesis”) and “antiemetic drugs” OR “antiemetic medication” (including “Neurokinin-1 receptor antagonists,” “antihistamines,” “anticholinergics,” and “corticosteroids”). Manual search helped to supplement database search for all eligible articles.
2.5. Data Collection Process
The researcher extracted data using a predesigned standardized table. The information assessed included author and year of publication, study design, participants, surgery type, anesthesia, intervention, and outcome.
2.6. Data Items
The primary outcome evaluated was the incidence of PONV cases after 24 hours of postoperative surgery. Also, the study assessed various secondary outcomes, such as complete response (CR) demonstrated by numerous metrics, such as lack of vomiting and no requirement for either antiemetic or rescue medication for surgical patients. Apart from the complete response, other types of secondary outcomes assessed were signs of vomiting and nausea within the first 24 hours following a surgical operation and the requirement of rescue and antiemetic medication among the patients.
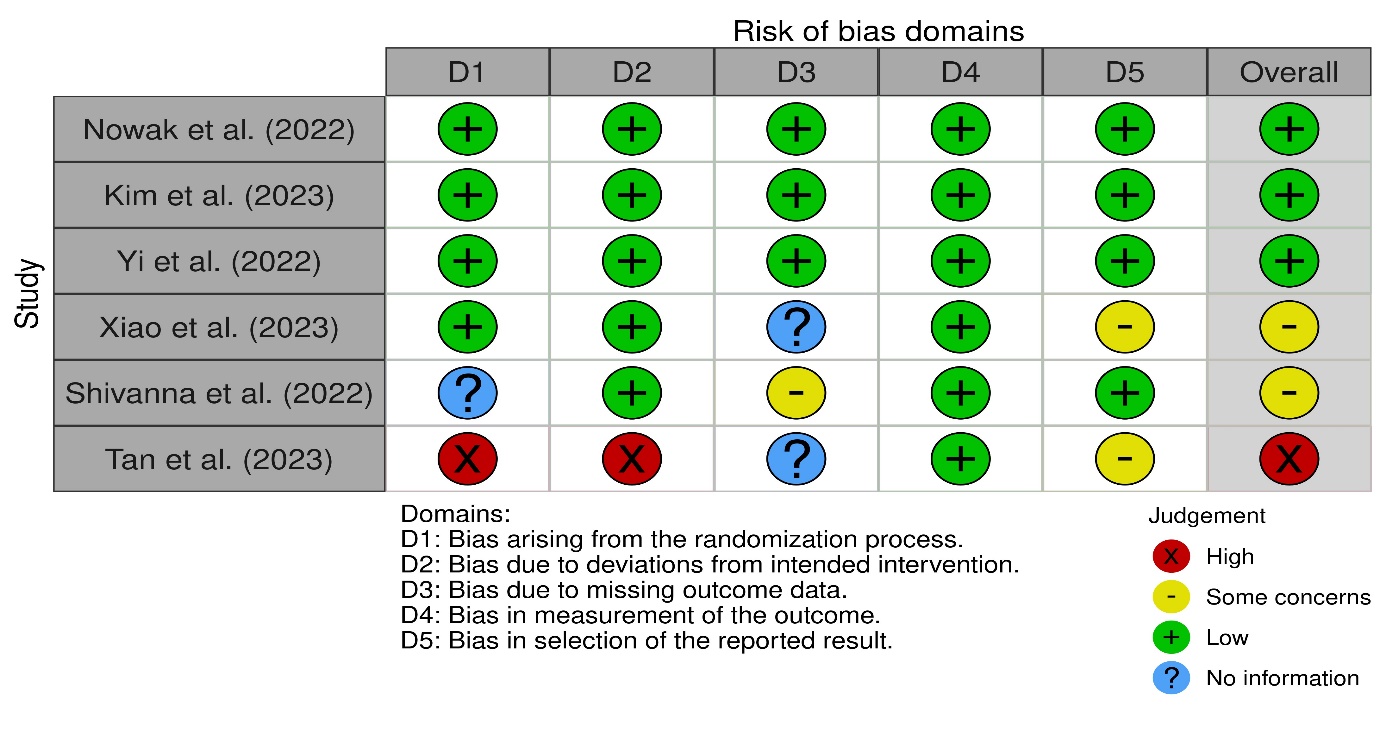
2.7. Risk of Bias in Individual Studies
The Cochrane Collaboration tool was critical in evaluating the quality of studies included in this research. Developed in 2008 and updated in 2011, the Cochrane Collaboration tool has been instrumental in determining the risk of bias in RCTs. According to Jørgensen et al., “The tool is based on seven domains: sequence generation and allocation concealment (both within the domain of selection bias or allocation bias), blinding of participants and personnel (performance bias), blinding of outcome assessors (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and an auxiliary domain: ‘other bias.’”9 The bias is either judged as unclear, low, or high.
2.8. Summary Measures
A meta-analysis was conducted using a random-effects model to account for the heterogeneity between studies. The data analysis involved calculating the odds ratio (OR) at 95% confidence interval (CI). This comprehensive and stringent methodological approach was critical for better understanding the role and effectiveness of pharmacological interventions in managing PONV.
2.9. Synthesis of Results
As already stated, odds ratios were calculated at 95% CI to examine the effectiveness of antiemetic drugs in ameliorating the adverse effects of PONV.
2.10. Risk of Bias Across Studies
The Cochrane Collaboration tool (https://www.bmj.com/content/343/bmj.d5928) was used to evaluate the eligibility and quality of the identified studies. The results were either unclear, low, or high among the assessed studies.
3.0. Results
3.1. Study Selection
A preliminary search of data in the three databases led to the retrieval of 1789 studies. After removing the duplicate records, only 1106 articles remained. These records were subjected to detailed screening using the inclusion and exclusion criteria, resulting in 6 studies that were included for synthesis. The PRISMA diagram (Figure 1) shows the criteria for selecting the desired articles for this study.

3.2. Study Characteristics
Table 1 documents the characteristics of the 6 studies included in this study. All the studies included either used the randomized-controlled trial or cohort design. The patient population underwent different surgeries, including gynecological, breast, urologic, orthopedic, rhinology, orthognathic, and elective surgery. All the patients were subjected to general anesthesia to facilitate the operations. Different antiemetic drugs were administered in the intervention group, including dexamethasone, droperidol, ondansetron, metoclopramide, dimenhydrinate, and ramosetron.
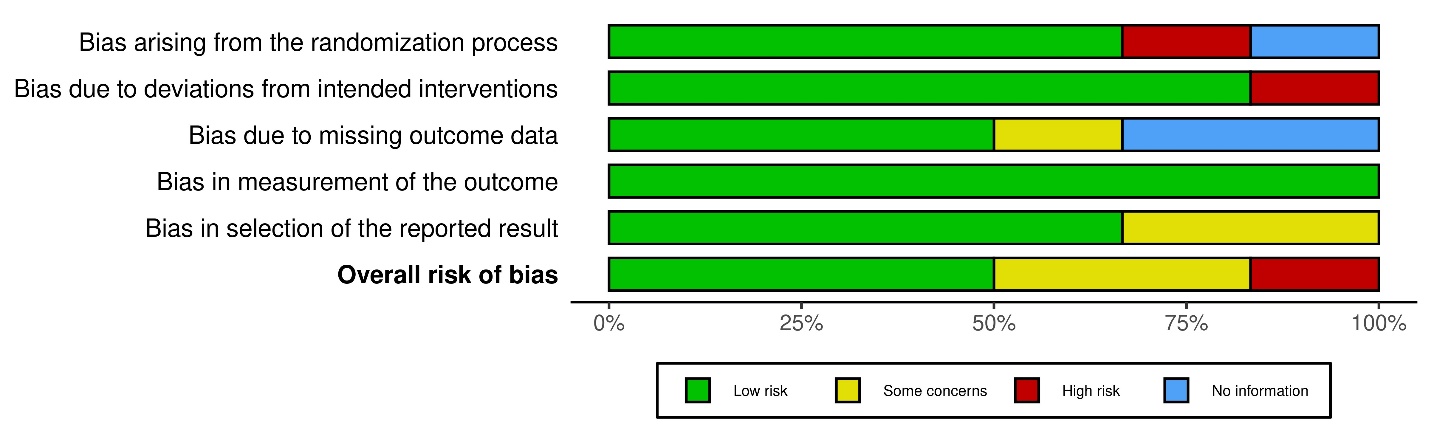
3.3. Risk of Bias Within Studies
The Cochrane Collaboration tool was utilized to examine the eligibility of the six identified studies. The quality analysis is demonstrated below.


3.4. Results of Individual Studies
3.4.1. Incidence of PONV
The following table summarizes the incidence of PONV in the individual studies after applying the intervention and the placebo.
Using the random effects model to conduct a pooled analysis of the 6 studies showed that PONV incidence for the experimental group was (OR 0.37, 95% CI: 0.28:0.40, P <.05). The low odds ratio means that there is a low likelihood of PONV occurring or being severe after using an antiemetic drug.
3.4.2. Incidence of Vomiting
All six studies reported the incidence of vomiting for patients undergoing surgical operations under anesthesia. However, after the use of antiemetic drugs, the studies reported a significant drop in postoperative nausea and vomiting complications. For instance, Shivanna et al. observed that a significant number of patients manifested signs and symptoms of vomiting between 0 and 6 hours after breast surgeries.12 This incidence was even higher in the O group, which had received a single dose of ondansetron, compared to the OD group, which received a combination of ondansetron and dexamethasone. However, none of the patients demonstrated vomiting after 12-24 hours. These findings were similar to Kim et al., who reported that none of the patients clinically manifested vomiting within the first 48 hours after taking a dose of ramosetron or a combination of ramosetron and dexamethasone.11 These findings highlight the efficacy of antiemetic medications in alleviating vomiting, particularly between 12-48 hours after the operation.
3.4.3. Incidence of Nausea
In the 2 studies that evaluated the incidence of nausea, the pooled analysis indicated that nausea was less severe in the intervention group compared to the placebo. Shivanna et al. found that none of the patients experienced nausea between 12 and 24 hours.12 Likewise, Kim et al. reported that the incidence of nausea within the first 1 hour after surgery was significantly lower in the experimental groups R and DR than in the control group C.11 However, no significant differences in nausea severity between the three groups could be observed between 0-48 hours.
3.4.4 Use of Rescue Antiemetic Drugs
All the studies evaluated the efficacy of either single or multiple antiemetic drugs in ameliorating the adverse signs and symptoms of PONV for patients undergoing anesthesia. All the studies reported significant inter-group differences, with the intervention groups demonstrating lower PONV incidence than the control and placebo groups. The rescue medications were more effective when combined than when used alone. For instance, Yi et al. established that PONV incidence for PACU patients was 14.5% for the group administered with dexamethasone and droperidol, 26.7% for the patients who received dexamethasone combined with tropisetron, and 50% for the control group that received dexamethasone alone.13 These findings were justified by Shivanna et al., who found that PONV incidence for patients administered with ondansetron alone was 38.9% and 11.1% within the first 6 and 12 hours, respectively.12 These incidences are slightly higher compared to the group administered with ondansetron and dexamethasone, which recorded 13.9% and 2.8% within the first 6 and 12 hours, respectively.
3.5. Synthesis of Results
The results of this systematic review show that the use of antiemetics for anesthetic patients after a surgical operation is critical in reducing the incidence of PONV. Tan et al.established that after administering droperidol to the experimental group, only 67 patients, translating to 12.1%, developed PONV.14 In contrast, in the control group, 120 patients, representing 21.1%, developed PONV, demonstrating the efficacy of the rescue medications. Further, studies revealed that administering antiemetic medications alleviates severe symptoms of PONV complications, including nausea and vomiting.11,12 The antiemetics are more effective when used in combination than when used alone. For example, Kim et al. reported that the incidence of nausea within the first 48 hours after surgery was 16% in experimental group R and 9% in intervention group DR.11 It is worth noting that participants in the former experimental group were administered with ramosetron alone, while those in DR were treated with ramosetron and dexamethasone. Besides, some classes of antiemetic drugs are more effective than others. Yi et al. found that the incidence of PONV was much lower in experimental group DD (14.5%) than in intervention group DT (26.7%). Patients in DD were treated with droperidol, while those in DT received tropisetron.13
4.0. Discussion
An extensive body of research documents that PONV prevalence is about 20-50%4 and that approximately 30% of patients develop post-discharge PONV.16 Despite the widespread efforts to establish both pharmacologic and non-pharmacological interventions, PONV remains a persistent clinical problem, which increases dramatically to as high as 80% for patients who are considered at high risk.4 Our study established that the use of antiemetic drugs can play a fundamental role in solving the persistent challenges associated with PONV complications. Noticeably, this study established that different types of antiemetic drugs, such as droperidol, tropisetron, dexamethasone, and ondansetron, among others, are effective in alleviating the adverse symptoms of PONV. Notably, these drugs are more efficient when utilized in combination with one another than when used alone. For example, combining ramosetron with dexamethasone increases their efficacy than when ramosetron is used alone.11 Furthermore, some types of antiemetics are more effective than others. Yi et al. reported that patients treated with droperidol show better outcomes than those administered with tropisetron.13 Therefore, healthcare professionals must choose more effective rescue medications, especially in cases where patients demonstrate severe PONV symptoms.
Our study had numerous limitations. First, it included patients subjected to different anesthesia and surgical operations. Second, the control group included patients given either saline or antiemetic medications that functioned via different mechanisms. Third, using studies done in English and published in the last five years posed a significant limitation since it excluded literature from studies available in other languages and those a bit older that might contain rich and useful information.
5.0. Conclusion
Even though antiemetic drugs have been widely accepted in treating PONV, their efficiency differs due to numerous factors, emphasizing the need for this systematic review to guide clinical decisions and enhance patient outcomes. This study revealed that all antiemetic drugs are effective in reducing the adverse clinical signs and symptoms of PONV. However, their efficacy differs from one rescue medication to another. These findings provide supportive and practical evidence for informing future clinical treatment guidelines for patients with postoperative nausea and vomiting after undergoing surgeries under anesthesia.